Chronic hepatitis B is a clinically silent and indolent disease with a long period of latency before significant adverse outcomes manifest, such as cirrhosis, decompensated liver disease, or hepatocellular carcinoma.[1] The hepatitis B virus (HBV) is not directly cytopathic to hepatocytes; the disease occurs when recurrent cycles (flares) of immune-mediated inflammation and liver injury result in the abnormal formation of collagenous scar or fibrosis that progresses over time.[2] The vast majority of individuals with HBV infection remain without symptoms or clinical manifestations unless cirrhosis-related complications develop; however, cirrhosis, in its asymptomatic form, is often unrecognized.[2] A clinician’s ability to detect cirrhosis is also limited by the absence of a readily accessible, sufficiently sensitive and well-validated biomarker or test to detect cirrhosis.[3] In the following discussion, we will review the goals for HBV treatment and the clinical indications for initiating antiviral therapy for chronic HBV. For the purposes of initiating HBV treatment, most experts and guidelines define chronic HBV infection as the presence of hepatitis B surface antigen (HBsAg) for at least 6 months.[4]
- Module 2 Overview
Treatment of HBV - Lesson 1
When to Initiate HBV TreatmentActivities- Lesson 2
Choosing an Initial HBV Treatment RegimenLesson 1. When to Initiate HBV Treatment
Learning Objective Performance Indicators
- Describe primary goals of therapy for the treatment of chronic HBV infection
- Name three key factors to consider when initiating treatment for chronic HBV infection
- List the four phases of immune responses that characterize HBV infection
- Summarize key recommendations in major guidance documents regarding when to initiate HBV treatment
- Discuss the clinical circumstances that warrant antiviral therapy in persons with chronic HBV infection for whom therapy may not be indicated
Last Updated: October 8th, 2024Author:H. Nina Kim, MD, MScH. Nina Kim, MD, MSc
Professor of Medicine
Division of Allergy & Infectious Diseases
University of WashingtonDisclosures: NoneReviewer:David H. Spach, MDDavid H. Spach, MD
Professor of Medicine
Division of Allergy & Infectious Diseases
University of WashingtonDisclosures: NoneTable of ContentsBackground
Goals of Therapy with Treatment of Chronic HBV
When considering treatment for persons with chronic HBV, it is important to consider the following goals of therapy.
- Immediate Goal: The most immediate goal for the treatment of persons with chronic HBV is to reduce hepatic inflammation (as measured by serum aminotransferases, ALT and AST) and to achieve virologic suppression, as indicated by plasma HBV DNA levels below the limit of detection.
- Intermediate Goal: With sustained virologic suppression and normalization of ALT, additional intermediate goals should include improvement in serologic and histologic markers. For hepatitis e antigen (HBeAg)-positive persons, the loss of HBeAg and change of antibody to HBeAg (anti-HBe) from negative to positive is referred to as “HBeAg seroconversion” and indicates reduced intrahepatic HBV replication, and portends a more favorable prognosis. With sustained virologic suppression, it is expected that persons with chronic HBV will also have hepatic histologic improvement, manifested by histologic evidence of regression of inflammation and fibrosis on liver biopsy.[5]
- Long-Term Goals: The ultimate and most important goal for treating persons with chronic HBV is to prevent the clinical complications of this infection, which include cirrhosis, hepatocellular carcinoma, and liver-related mortality.
- Prevention of HBV Transmission: When treating pregnant mothers with HBV DNA levels greater than 200,000 IU/mL, the primary goal is to prevent HBV transmission to the infant.[6] In addition, treatment of adults with chronic HBV may reduce sexual and injection-drug related transmission of HBV to another person who does not have HBV, but this is not usually considered a primary prevention strategy since HBV vaccination is a more reliable and proven means of protecting persons at risk of acquiring HBV.
- Control Rather than Eradication of HBV: The eradication of HBV is not currently feasible with existing antiviral therapy and thus HBV treatment is not considered curative but rather disease-modifying.[1] This viral persistence is thought to be due in part to the stability of the HBV genome and its incorporation into the hepatocyte nucleus in the form of covalently closed circular (ccc) DNA.[1,5,7] Notably, loss of hepatitis B surface antigen (spontaneously or with antiviral therapy) does not necessarily indicate complete HBV eradication.[1] For example, HBV reactivation can still occur in some individuals with isolated hepatitis B core antibody (anti-HBc) who are treated with immunosuppressive, cytotoxic, or biologic disease-modifying antirheumatic drugs.[8,9,10]
Factors Used to Determine Whether to Initiate Treatment
Because of the dynamic nature of HBV infection, our inability to eradicate HBV, and the potentially long, if not indefinite, duration of therapy (as in the case of oral nucleoside or nucleotide analogues), treatment is not universally indicated for everyone with chronic HBV, but rather reserved for those who are thought most likely to benefit from the standpoint of disease modification. Conceptually, the clearest indications for treatment are when significant liver fibrosis has occurred and/or when there is active HBV DNA replication along with sustained hepatic inflammation. The decision to treat persons with chronic HBV therefore typically incorporates the following three factors: (1) fibrosis status assessed by either non-invasive methods or biopsy, (2) evidence of hepatic inflammation, as measured by alanine aminotransferase (ALT) levels (or less commonly liver biopsy), and (3) ongoing HBV replication as indicated by serum HBV DNA levels. Some guidelines incorporate the HBeAg status as another parameter to consider in deciding whether to initiate HBV treatment. In addition to these criteria, there are special conditions for which treatment of chronic HBV would be advised even if the patient does not have an indication based on the presence of significant fibrosis and/or hepatic inflammation; these conditions will be discussed briefly as well.
Presence of Moderate Disease or Significant Fibrosis
There is now consensus among the major hepatitis treatment guidelines (American Association for the Study of Liver Diseases [AASLD], European Association For The Study Of The Liver [EASL], Asian Pacific Association for the Study of the Liver [APASL], and the World Health Organization [WHO]) that the presence of at least moderate liver necroinflammation or fibrosis warrants initiation of HBV treatment.[4,11,12,13] Moderate or significant fibrosis has historically been defined by the gold standard of liver biopsy and the presence of METAVIR stage F2 fibrosis. However, given the risks and limited accessibility/acceptability of biopsy, noninvasive measures are considered reasonable alternatives when biopsy is not feasible.[4,12] Among these major HBV treatment guidelines, the 2024 WHO guidelines directly address the threshold of significant fibrosis by AST-platelet ratio index (APRI) or transient elastography.[13]
Cirrhosis Status
Individuals with chronic HBV and cirrhosis are at much greater risk of liver-related morbidity and mortality than persons without cirrhosis. The 5-year cumulative risk of hepatocellular carcinoma, for example, is estimated to be 10- to 15-fold higher in patients with cirrhosis than those without.[14] The evidence base for the beneficial impact of HBV-active antiviral therapy on reducing the risk of adverse clinical outcomes, such as hepatic decompensation or hepatocellular carcinoma (HCC), is particularly compelling for patients with cirrhosis.[15] The presence of cirrhosis is generally considered a strong indicator that favors initiating HBV treatment.
Evaluation of Cirrhosis Status
Since cirrhosis is a strong indication for HBV treatment, it is important to evaluate persons with chronic HBV for the presence of cirrhosis. A detailed discussion of Evaluation and Staging of Liver Fibrosis can be found on the Hepatitis C Online site. Current guidelines do not directly address the best method for identifying cirrhosis in patients with chronic HBV. The following provides a brief summary regarding the evaluation of cirrhosis in a person with chronic HBV infection, including invasive testing that can establish a definitive diagnosis (liver biopsy) and noninvasive tests that make a presumptive diagnosis (transient elastography, hepatic ultrasound, and laboratory markers). Ultimately, as with many diagnoses, the determination of cirrhosis typically relies on an overall appraisal of multiple clinical parameters, as well as pre-test probability.
- Clinical Features: Since many persons can develop cirrhosis without obvious clinical findings, the physical examination should not be used to rule out cirrhosis. Nevertheless, the presence of obvious manifestations of cirrhosis on physical examination, such as ascites, jaundice, spider angiomata, splenomegaly, or encephalopathy, are important to evaluate and can increase the likelihood of a cirrhosis diagnosis.
- Liver Biopsy: A liver biopsy remains the gold standard for determining disease severity in chronic HBV and provides a direct assessment of inflammatory activity and degree of fibrosis. Cirrhosis is thus a histologic diagnosis, and refers to an advanced stage of fibrosis that has extended beyond the portal triad to form bridges of scar that eventually results in the distortion of hepatic architecture. Liver biopsy can have limitations, including under-sampling and misclassification.[16] Liver biopsy is also invasive and although the risk of complications, such as intrahepatic bleeding or biliary injury, is very low, liver biopsy is recommended only for a subset of patients with chronic hepatitis B.[16]
- Transient Elastography: Transient elastography offers reasonably high diagnostic accuracy in detecting cirrhosis, but estimations of liver stiffness, the measurement of elastography, can be confounded by the presence of significant hepatic necroinflammation.[17]
- Hepatic Ultrasound: Ultrasonography is often used in clinical practice for staging chronic viral hepatitis. While it can have high specificity for detecting cirrhosis if a small nodular liver and signs of portal hypertension (e.g., splenomegaly) are present, its sensitivity for detecting advanced fibrosis can be suboptimal.[18,19]
- Laboratory Markers: Assessment of liver disease severity also includes laboratory evaluation of complete blood count with platelet count, serum aminotransferase levels (ALT and AST), alkaline phosphatase, bilirubin, serum albumin, and prothrombin time. Gradual decline in serum albumin in conjunction with gradual increase in alkaline phosphatase or prothrombin time without other explanation may signal cirrhosis. In viral hepatitis, ALT typically exceeds AST but with advanced fibrosis, this ratio often reverses. The Fibrosis 4 (FIB-4) score is based on AST/ALT ratio, platelet count, and age; the actual Fib-4 score can be determined with a Fib-4 Calculator and this score has been shown to have reasonable performance in differentiating mild (stage 0-1) from more advanced (stage 3-4) fibrosis in chronic hepatitis B that is not being treated.[20,21]
Decompensated Cirrhosis
Persons with cirrhosis are considered to have decompensated cirrhosis if certain liver-related complications develop, including jaundice, ascites, esophageal variceal bleeding, hepatic encephalopathy, or impaired hepatic synthetic function (as reflected by elevated prothrombin time or total bilirubin). Decompensated cirrhosis is often defined as a Child-Turcotte-Pugh score of 7 or greater (class B or C). Because antiviral therapy has been shown to improve transplant-free survival in patients with decompensated cirrhosis, they should also be started on oral antiviral therapy regardless of ALT or HBV DNA levels. Patients with more advanced disease should also be referred for liver transplantation, if eligible.
Serum HBV DNA Level
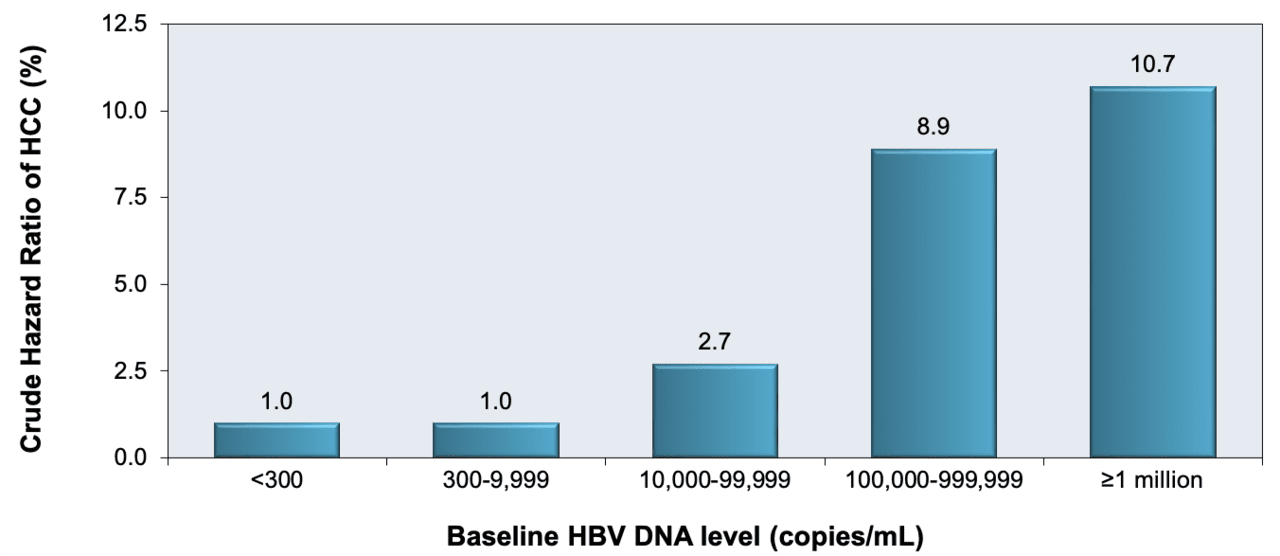
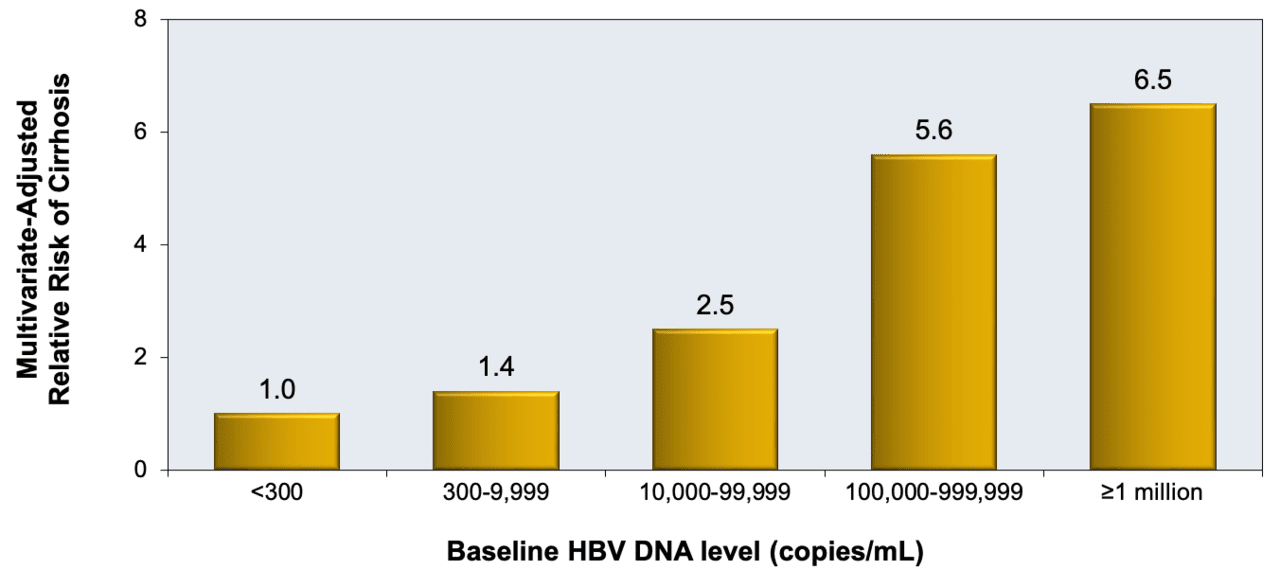
Because there can be a lack of correlation between ALT and disease activity when examined on its own, ALT must be considered in conjunction with the serum HBV DNA level.[22,23] In the large prospective REVEAL cohort study, investigators enrolled 3,653 persons 30 to 65 years of age in Taiwan, and followed them for a mean of 11.4 years; when compared with those with HBV DNA levels less than 10,000 copies/mL (approximately 2,000 IU/mL), the risk of liver cancer was shown to range from 2.7-fold higher in those with a serum HBV DNA level of 10,000 to 99,999 copies/mL (approximately 2,000 to 20,000 IU/mL) to 10.7-fold higher in those with a HBV DNA level greater than or equal to 1 million copies/mL (greater than or equal to approximately 200,000 IU/mL) (Figure 1).[24] This landmark study provided the early proof of concept for serum HBV DNA levels as a major driver of disease pathogenesis and the possibility of HBV suppression as a key intervention in mitigating disease progression.[24] In a separate but similar study, persons with chronic HBV were also found, in a dose-dependent gradient, to have an increased risk of cirrhosis with increasing serum HBV DNA levels, with a notable 6.5-fold higher risk in those with HBV DNA levels greater than 1 million copies/mL (approximately 200,000 IU/mL) compared with those with a HBV DNA level less than 300 copies/mL (less than approximately 60 IU/mL) (Figure 2).[25]
Alanine Aminotransferase (ALT) Levels
Serum ALT levels provide a rapid and noninvasive measure that can indicate hepatic inflammation. In 2002, investigators suggested using upper limits of normal for ALT levels of greater than 19 U/L in women and 30 U/L in men as the recommended cutoffs to accurately identify those with underlying hepatitis C viremia. Subsequently, the American Association for the Study of Liver Diseases (AASLD) hepatitis B guidelines suggest using the same threshold values as the upper limit of normal for ALT levels.[26,27,28] The 2018 AASLD Hepatitis B Guidance, however, changed the upper limit of normal for treatment purposes to 25 U/L for women and 35 U/L for men.[4] These cutoffs are lower than the upper limit of normal defined by many commercial laboratories, which derive their range from the general population and more specifically from blood donors without evidence of hepatitis B or hepatitis C infection. Due to the high prevalence of fatty liver in "healthy" donors (who may have elevated ALT levels), use of the upper limit of normal obtained from these donor pools may not maximize detection of individuals with underlying liver disease due to viral hepatitis.[29] Therefore, even though a patient may have a “normal” ALT result as defined by a reference laboratory, the more stringent cutoffs would reduce the likelihood of missing underlying liver disease caused by hepatitis B. It is also important to note that a treatment decision should not be made on the basis of a single serum ALT measurement. These values often vary, and the phase of HBV infection will need to be confirmed with multiple measurements of serum ALT over time, typically drawn every 3 to 6 months, particularly given the dynamic nature of HBV infection.
Immune Phases of Chronic HBV Infection
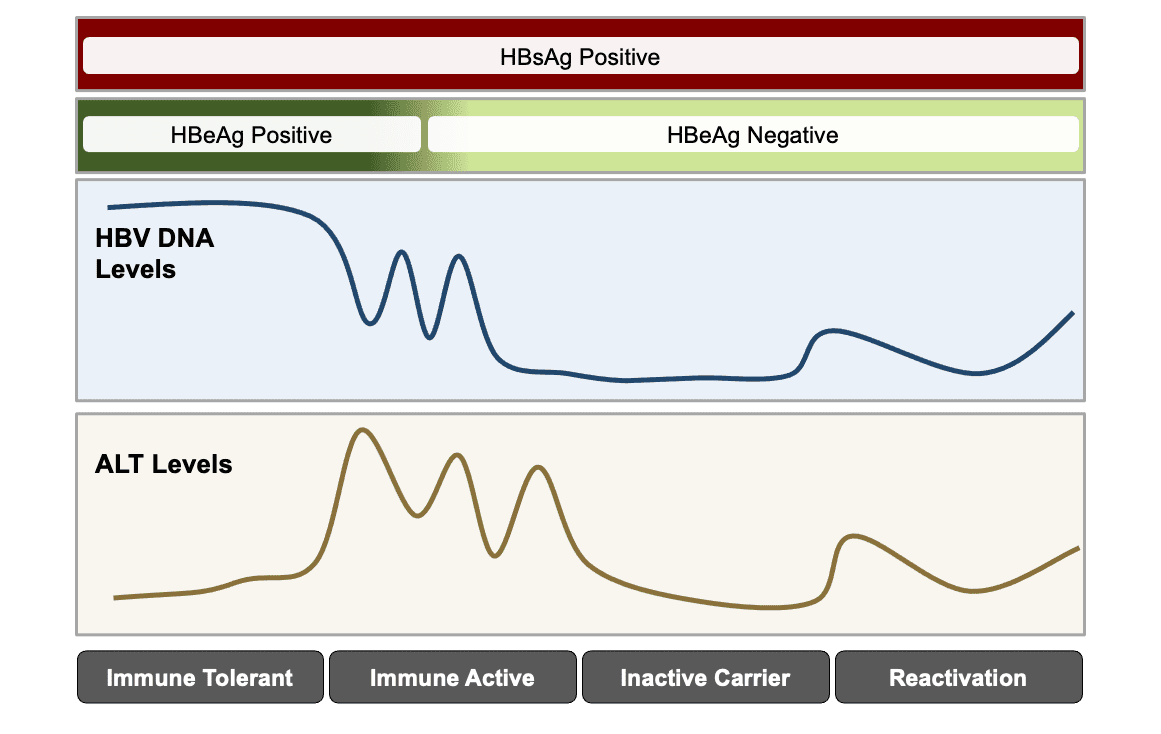
From a conceptual standpoint, chronic HBV infection has been characterized by four phases (or types of immune responses): immune tolerant, immune active, inactive carrier, and reactivation.[30,31,32,33] The liver damage that can occur with chronic HBV infection is primarily related to the host immune response to hepatocytes infected with HBV; the inflammation and liver cell death associated with this immune response is thought to occur predominantly in the immune-active phase of chronic HBV. The phases of chronic HBV infection are not considered static—individuals can undergo transitions in and out of these different stages throughout their lifetime (Figure 3).[4,31]
Immune-Tolerant Chronic HBV
The AASLD characterizes the immune-tolerant phase as one with a positive HBeAg, very high HBV DNA levels (typically greater than 1 million IU/mL), normal or minimally elevated ALT and/or AST levels, and liver biopsy (if done) showing no fibrosis and minimal inflammation.[4] Despite having very high HBV DNA levels, there is little immune reaction to the virus-infected hepatocytes and minimal liver inflammation. Also, these individuals do not tend to respond well to oral antiviral therapy or peginterferon.[34] Thus, persons in the immune-tolerant phase are not generally considered candidates for therapy unless they meet specific age and/or histologic criteria. These individuals should have their ALT monitored every 6 months to assess for transition to immune-active infection.[4] However, studies have shown that up to one-third of persons with chronic HBV who are older than 40 years of age with normal ALT can have significant inflammation (grade 2 or higher) and/or fibrosis (stage 2 or higher). In these patients, normal ALT can be a less reliable predictor of quiescent or minimal disease.[35,36]
Immune-Active Chronic HBV or Reactivation of Chronic HBV
The AASLD defines immune-active chronic HBV as persistent elevation of ALT at least 2 times greater than the upper limit of normal (or evidence of significant histologic disease) plus elevated HBV DNA above 2,000 IU/mL if HBeAg negative or above 20,000 IU/mL if HBeAg positive.[4] If this occurs in HBeAg-negative persons after a period in the inactive carrier phase, this has also been referred to as reactivation. For persons who do not have cirrhosis or any special condition that warrants HBV treatment, the main indication for therapy would be evidence of immune activity, as reflected by persistent (at least 3 to 6 months) elevations in both ALT and plasma HBV DNA levels. The evidence to support the benefit of antiviral treatment in reducing the risk of clinical events (cirrhosis and HCC-related mortality) is found primarily in patients who have met criteria for immune-active disease.[15] These include observational studies as well as randomized controlled trials (RCTs) that compared a control group (no treatment or placebo) with either interferon-based therapy or an oral nucleoside or nucleotide analogue agent. Seven RCTs involving 3,463 patients followed for a mean of 28 months demonstrated that antiviral therapy significantly reduced the risk of decompensated liver disease and cirrhosis.[15] Further, in 35 observational studies of 59,201 patients followed for a mean of 60 months, antiviral therapy versus control was associated with a decreased risk of HCC, cirrhosis and all-cause mortality in this population.[15]
Inactive Chronic Hepatitis B
The AASLD characterizes inactive chronic HBV as an HBeAg-negative (and anti-HBe positive), status with serum HBV DNA levels less than 2,000 IU/mL, persistently normal ALT and/or AST levels, and liver biopsy that confirms absence of significant necroinflammation, and variable levels of fibrosis observed on liver biopsy or noninvasive testing.[4] These individuals are not usually considered candidates for therapy, but require ongoing monitoring for immune-active transition. In addition, these individuals can go on to HBV reactivation, either spontaneously or with immunosuppression. It is important to note that even inactive carriers with low HBV viral levels remain at risk for HCC.[35,37] Therefore, guidelines recommend these patients also undergo HCC screening when indicated.
Hepatitis B Treatment Guidance Recommendations
Several leading professional organizations have provided guidance on when to initiate treatment for persons with chronic HBV. [4,11,12] The following summary is intended to provide a succinct description of their recommended indications for initiating HBV treatment. The reader is encouraged to access these original documents for additional details, discussion, and information about the level of evidence and strength of recommendations
.Table 1. HBV Treatment Recommendation Based on Major Organization Guidelines
Risk Group AASLD
2018APASL
2015EASL
2017WHO
2024Without cirrhosis
Treat if:
- ALT ≥2x ULN1, or
- Significant histologic disease2
and
- HBV DNA >2000 IU/mL if HBeAg-negative
- HBV DNA >20,000 IU/mL if HBeAg-positiveTreat if:
- ALT >2x ULN3, or
- Significant histologic disease3
and
- HBV DNA >2000 IU/mL if HBeAg-negative
- HBV DNA >20,000 IU/mL if HBeAg-positiveTreat if:
- ALT >40 IU/L, HBV DNA >2,000 IU/mL, and biopsy evidence of at least moderate necroinflammation or fibrosis, or
- HBV DNA >2,000 IU/mL and biopsy evidence of at least moderate fibrosis, or
- HBV DNA >20,000 IU/mL and ALT > 2x ULN3 regardless of degree of fibrosisTreat if any:
- Significant fibrosis5
- Coinfection with HCV, HDV, or HIV
- Family history of liver cancer or cirrhosis
- Comorbidities
- Immune suppression
- Extrahepatic
- Persistent abnormal ALT6Compensated cirrhosis
Treat all4
Treat if:
- HBV DNA >2,000 IU/mL, or
- ALT elevated3Treat all4
Treat all4 Decompensated cirrhosis
Treat all4 and refer for liver transplantation Treat all4 Treat all4 Treat all4
Abbreviations: ASLD = American Association for the Study of Liver Diseases; APASL = Asian Pacific Association for the Study of the Liver; EASL= European Association for the Study of the Liver; WHO = World Health Organization; ALT = alanine aminotransferase; ULN = upper limit of normal
1Regardless of HBV DNA, ALT, or HBeAg status; 2Upper limit of normal, defined as ALT 35 IU/L for men, 25 IU/L for women; 3Defined as ALT 40 IU/L for both men and women; 4Defined as at least moderate necroinflammation or at least moderate fibrosis according to histopathologic grading/staging; 5The thresholds for significant fibrosis by APRI or transient elastography have not been fully validated in adolescents; 6Defined as two ALT values greater than 19 IU/L for women and 39 IU/L for men at unspecified intervals during a 6- to 12-month period.Source:- European Association For The Study Of The Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67:370-98. [PubMed Abstract]
- Sarin SK, Kumar M, Lau GK, et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 update. Hepatol Int. 2016;10:1-98. [PubMed Abstract]
- Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67:1560-99. [PubMed Abstract]
- World Health Organization. Guidelines for the prevention, diagnosis, care and treatment for people with chronic hepatitis B infection. March 29, 2024. [WHO]
American Association for the Study of Liver Diseases (AASLD)
The American Association for the Study of Liver Disease (AASLD) hepatitis B guidance has served as the main HBV treatment guidance in the United States. The recommendations in the AASLD 2018 Hepatitis B Guidance were developed after literature review and by an expert panel (gastroenterology and hepatology).[4,26] The most recent version of this guidance was published in 2018 as an update to the 2016 AASLD Guidelines, with the prior 2016 version having a more formal evidence review.[4,26] The 2016 and 2018 AASLD Hepatitis B Guidance recommends initiating HBV treatment in the following situations in persons with chronic HBV.[4,26]
- Immune-Active Disease: Treatment is recommended for persons with immune-active disease. For treatment purposes, immune-active disease is defined as (1) elevation of ALT (at least 2 times the upper limit of normal) or evidence of significant histologic disease and (2) elevated HBV DNA above 2,000 IU/mL if HBeAg negative or above 20,000 IU/mL if HBeAg positive. The AASLD recommends using an ALT upper limit of normal of 35 U/L for males and 25 U/L for females to guide management decisions. Notably, neither the 2016 nor the 2018 AASLD guidance discusses the duration of ALT elevation to be counted as a persistent (rather than isolated) finding, but the preceding 2009 guidelines discuss using a period of 3 to 6 months. Significant histologic disease is defined as at least moderate necroinflammation and/or fibrosis.
- Compensated Cirrhosis: Treatment is recommended for all persons with cirrhosis, regardless of HBV DNA level, HBeAg status, or ALT levels.
- Decompensated Cirrhosis: Initiation of oral antiviral treatment is recommended in conjunction with referral for consideration of liver transplantation.
- Selected Older Patients: Treatment is recommended in the select group of adults older than 40 years of age who have normal ALT levels, elevated HBV DNA (1,000,000 IU/mL) levels, and a liver biopsy specimen that shows significant necroinflammation or fibrosis.
Asian Pacific Association for the Study of the Liver (APASL)
The Asian Pacific Association for the Study of the Liver (APASL) hepatitis B guidance was generated by a panel of experts in this region, predominantly from the specialties of hepatology and gastroenterology. The most recent APASL Hepatitis B Guidance was published in 2015.[11] The 2015 APASL Hepatitis B Guidelines recommend initiating HBV treatment in the following situations for persons with chronic HBV.[11]
- Without Cirrhosis: Treatment may be started in noncirrhotic patients who have (1) persistent elevation of ALT (greater than 2 times the upper limit of normal at least 1 month between tests) and (2) elevated HBV DNA above 2,000 IU/mL if HBeAg negative or above 20,000 IU/mL if HBeAg positive. The ALT upper limit of normal used to guide management decisions is 40 U/L for both males and females. In addition, patients who have evidence of at least moderate inflammation and/or significant fibrosis on biopsy should also be considered for therapy regardless of ALT or HBV DNA level. Moderate inflammation is defined as either an Ishak activity score greater than 3 (out of a possible 18 total) or a METAVIR activity score of A2 or A3; significant fibrosis means F2 or greater by METAVIR fibrosis score or Ishak fibrosis stage of 3 or greater.
- Compensated Cirrhosis: Treatment is recommended with (1) HBV DNA level greater than 2,000 IU/mL regardless of ALT level or HBeAg status, or (2) any detectable HBV DNA level if ALT elevated, regardless of HBeAg status.
- Decompensated Cirrhosis: Treatment is recommended with any detectable HBV DNA level, regardless of ALT levels or HBeAg status.
European Association for the Study of the Liver (EASL)
The European Association for the Study of the Liver (EASL) hepatitis B clinical practice guidelines is the major hepatitis B guidance for Europe and this document was primarily written by gastroenterology and hepatology specialists.[12] The EASL Hepatitis B Clinical Practice Guidelines recommend initiating HBV treatment in the following situations.[12]
- Without Cirrhosis
- Treatment is recommended regardless of HBeAg status if (1) the HBV DNA level is greater than 2,000 IU/mL, (2) the ALT is greater than the upper limit of normal (approximately 40 IU/L for males and females), and (3) there is liver biopsy evidence of at least moderate liver necroinflammation and/or at least moderate fibrosis.
- Treatment is recommended regardless of ALT levels or HBeAg status if (1) the HBV DNA level is greater than 2,000 IU/mL and (2) there is liver biopsy evidence of at least moderate fibrosis (based on liver biopsy or noninvasive markers of fibrosis).
- Treatment is recommended regardless of HBeAg status if (1) the HBV DNA level is greater than 20,000 IU/mL and (2) the ALT is greater than 2 times the upper limit of normal (approximately 40 IU/L for males and females), regardless of the degree of fibrosis.
- Compensated Cirrhosis: Treatment is recommended with any detectable HBV DNA level, regardless of ALT levels or HBeAg status.
- Decompensated Cirrhosis: Treatment is recommended with any detectable HBV DNA level, regardless of ALT levels or HBeAg status.
- Selected Indications: These guidelines also note that treatment can be offered, even in the absence of preceding indications for:
- HBeAg-positive persons older than 30 years of age with persistently normal ALT and high HBV DNA levels, regardless of the severity of liver histology.
- Persons with a family history of hepatocellular carcinoma, cirrhosis, or extrahepatic manifestations.
World Health Organization (WHO)
In 2024, the World Health Organization issued an update to their comprehensive guidance on HBV prevention, care and treatment. Among the updates included expanded treatment eligibility that applies to all adults as well as adolescents aged 12 or older. Among the four main criteria for treatment outlined below, only one requires access to HBV DNA quantitation, which has been a major barrier to accessing treatment in more resource-limited settings.- Without Cirrhosis: Treat adult or adolescent ≥12 years if:
- Significant fibrosis defined as:
- APRI >0.5 or transient elastography >7.0 kPa, or
- HBV DNA level >2000 IU/mL and ALT ≥30 U/L for males, ≥19 U/L for females
- Presence of any of the following:
- Coinfection (HDV, HIV, HCV), or
- Family history of liver cancer or cirrhosis, or
- Immune suppression, or
- Comorbidities (e.g., diabetes, metabolic associated steatotic liver disease or MASLD), or
- Extrahepatic manifestations (e.g., glomerulonephritis, vasculitis)
- Significant fibrosis defined as:
- Persistently Abnormal ALT levels: Treatment is recommended with persistently abnormal ALT levels (defined as two ALT values of ≥19 for women or ≥30 I/U for men at unspecified intervals during a 6- to 12-month period).
- Cirrhosis: Treatment is recommended for all such individuals, regardless of HBV viral level.
- Decompensated Cirrhosis: Treatment is recommended for all such individuals, regardless of HBV viral level.
HBV Primary Care Workgroup
The HBV Primary Care Workgroup includes members in the United States from hepatology, infectious diseases, pharmacy, primary care, and public health.[38] The HBV Primary Care Workgroup Guidance was first released in early 2020 and is accessible on this web site (Hepatitis B Online).[38] The goal of this document is to provide simplified, up-to-date, and readily accessible HBV management guidance for primary care medical providers. Note, this guidance does not incorporate HBeAg status in the initial decision-making process, but persons positive for HBeAg are recommended to undergo monitoring of HBeAg for evidence of HBeAg seroconversion. The HBV Primary Care Workgroup Guidance recommends initiating HBV treatment in the following situations.[38]
- Without Cirrhosis: For persons without cirrhosis, treatment is recommended if the HBV DNA level is greater than 2,000 IU/mL and the ALT level is elevated, regardless of HBeAg status. For this purpose, elevated ALT is defined as greater than 25 U/L in females and greater than 35 U/L in males that is persistent for at least 3 to 6 months.
- Cirrhosis: Treatment is recommended for all persons with cirrhosis, regardless of HBV DNA level, ALT level, or HBeAg status.
- Decompensated Cirrhosis: Treatment is recommended but persons should be promptly referred to a hepatologist.
Special Indications for Initiating Treatment
There are a variety of special clinical situations in patients with HBV where antiviral therapy may be warranted regardless of cirrhosis status, hepatic aminotransferase levels, or HBV DNA levels.[4] The most common of these specific circumstances are listed below.
- Pregnant Women with an HBV DNA level Greater than 200,000 IU/mL: Treatment of HBV is indicated for all pregnant women with an HBV DNA level greater than 200,000 IU/mL in the third trimester of pregnancy.[4,6] The purpose of HBV treatment of a pregnant woman with a high HBV DNA level is to further reduce the risk of perinatal transmission beyond what is accomplished by passive and active HBV immunization given to the newborn.[39]
- Persons with HIV and HBV Coinfection: Fully suppressive antiretroviral therapy to treat HIV is recommended for all persons with HIV.[40] In addition, all persons with HIV and chronic HBV should receive concomitant treatment for HBV, regardless of the cirrhosis status, hepatic aminotransferase levels, or HBV DNA levels.[41] The goal of treating HBV in persons with HIV coinfection is to reduce the excess risk of liver-related morbidity and mortality that persons with HIV and HBV coinfection have (when compared to persons who have HBV monoinfection or HIV monoinfection).[42,43] Antiviral treatment should ensure concomitant fully active treatment for HIV and HBV, with a regimen that ideally includes three medications with activity against HIV and two medications with activity against HBV (typically tenofovir DF or alafenamide with emtricitabine or lamivudine).[41]
- Persons at Risk for HBV Reactivation: Individuals with untreated chronic HBV or past infection with HBV are at risk of HBV reactivation if they receive immunosuppressive, cytotoxic, or biologic disease-modifying antirheumatic drugs.[9,10,44] In this context, HBV reactivation is defined as either an increase in HBV DNA levels over baseline or seroreversion (from HBsAg-negative to HBsAg-positive). This reactivation results from loss of immune control of HBV, with potential high-level viral replication and resultant inflammatory activity or flare.[9,10] Reactivation of HBV can also occur in persons receiving HCV therapy with direct-acting antiviral agents (DAAs).[45,46] In any setting of increased risk of HBV reactivation, the primary goal of administering HBV antiviral therapy prior to immunosuppressive or HCV therapy is to reduce the risk of HBV reactivation and associated liver injury, which has the potential to be severe in this setting.[9,10] For more details on this topic, see the Lesson on HBV Reactivation in the Setting of Immunosuppression.
- Persons with Chronic HBV Receiving HIV Preexposure Prophylaxis: In the United States, two regimens are FDA-approved for HIV preexposure prophylaxis (PrEP): tenofovir DF-emtricitabine or tenofovir alafenamide-emtricitabine.[47,48] The use of HIV PrEP may be indicated in a person who also has chronic HBV infection. Since both of the oral medication combinations used for HIV PrEP are highly active against HBV, any person with chronic HBV who is receiving oral HIV PrEP is also receiving treatment for HBV. In contrast to the oral PrEP options, the long-acting injectable medication approved for HIV PrEP, cabotegravir, is not active against HBV. It is important to understand that any individual who intermittently takes the currently recommended oral HIV PrEP or goes on and off oral HIV PrEP could create unintended negative consequences related to the HBV infection, such as generation of HBV drug resistance or developing HBV-related hepatic flares. When oral HIV PrEP is used in persons with chronic HBV infection, it should include appropriate counseling related to the risks of oral HIV PrEP interruption, as well as clinical and laboratory monitoring if oral HIV PrEP is stopped.
Summary Points
- The goals of HBV treatment are to prevent the development of cirrhosis, hepatocellular carcinoma, and liver-related death.
- Antiviral therapy is not considered curative but can improve serologic, virologic, and histologic endpoints. It has also been shown to reduce the risk of liver-related outcomes such as cirrhosis and HCC in selected patients.
- Multiple organizations, including AASLD, EASL, APASL, and the WHO, have issued guidance that addresses treatment indications for persons with chronic HBV.
- According to these groups, antiviral therapy is indicated in all patients with chronic HBV and cirrhosis, regardless of ALT level.
- According to most guidelines, antiviral therapy is indicated in patients with chronic HBV without cirrhosis who meet the criteria for persistent immune-active disease, as defined by elevated HBV DNA level (greater than 2,000 IU/ML) and persistent elevated ALT levels.
- For the purpose of making treatment decisions in persons with chronic HBV infection, the AASLD guidance recommends using an upper range of normal ALT of 25 IU/L in women and 35 IU/L in men; the WHO ALT thresholds are 19 IU/L for women and 39 IU/L for men.
- Antiviral therapy for chronic HBV is indicated in patients who have evidence of at least moderate liver necroinflammation or fibrosis, determined traditionally by biopsy but now more often by non-invasive measures such as AST-platelet ratio index or transient elastography.
- Antiviral therapy for chronic HBV may be indicated regardless of the phase of disease in those patients who have a variety of special conditions that include pregnancy, immune suppression, and HIV coinfection.
- Other clinical factors such as age, family history of HCC, and comorbidities (i.e. extrahepatic manifestations) should be considered in the decision to treat or perform a biopsy on an individual with chronic HBV.
Citations
- 1.Likhitsup A, Lok AS. Understanding the Natural History of Hepatitis B Virus Infection and the New Definitions of Cure and the Endpoints of Clinical Trials. Clin Liver Dis. 2019;23:401-16.[PubMed Abstract] -
- 2.Chang ML, Liaw YF. Hepatitis B flares in chronic hepatitis B: pathogenesis, natural course, and management. J Hepatol. 2014;61:1407-17.[PubMed Abstract] -
- 3.Walker M, El-Serag HB, Sada Y, et al. Cirrhosis is under-recognised in patients subsequently diagnosed with hepatocellular cancer. Aliment Pharmacol Ther. 2016;43:621-30.[PubMed Abstract] -
- 4.Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67:1560-99.[PubMed Abstract] -
- 5.Dienstag JL. Hepatitis B virus infection. N Engl J Med. 2008;359:1486-500.[PubMed Abstract] -
- 6.Schillie S, Vellozzi C, Reingold A, et al. Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2018;67:1-31.[PubMed Abstract] -
- 7.Tu T, Budzinska MA, Shackel NA, Urban S. HBV DNA Integration: Molecular Mechanisms and Clinical Implications. Viruses. 2017;9.pii: E75.[PubMed Abstract] -
- 8.Querido S, Weigert A, Adragão T, et al. Risk of hepatitis B reactivation in hepatitis B surface antigen seronegative and core antibody seropositive kidney transplant recipients. Transpl Infect Dis. 2019;21:e13009.[PubMed Abstract] -
- 9.Sasadeusz J, Grigg A, Hughes PD, et al. Screening and Prophylaxis to Prevent Hepatitis B Reactivation: Other Populations and Newer Agents. Clin Liver Dis. 2019;23:521-34.[PubMed Abstract] -
- 10.Sasadeusz J, Grigg A, Hughes PD, et al. Screening and Prophylaxis to Prevent Hepatitis B Reactivation: Patients with Hematological and Solid Tumor Malignancies. Clin Liver Dis. 2019;23:511-9.[PubMed Abstract] -
- 11.Sarin SK, Kumar M, Lau GK, et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 update. Hepatol Int. 2016;10:1-98.[PubMed Abstract] -
- 12.European Association For The Study Of The Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67:370-98.[PubMed Abstract] -
- 13.World Health Organization. Guidelines for the prevention, diagnosis, care and treatment for people with chronic hepatitis B infection. March 29, 2024.[WHO] -
- 14.Raffetti E, Fattovich G, Donato F. Incidence of hepatocellular carcinoma in untreated subjects with chronic hepatitis B: a systematic review and meta-analysis. Liver Int. 2016;36:1239-51.[PubMed Abstract] -
- 15.Lok AS, McMahon BJ, Brown RS Jr, et al. Antiviral therapy for chronic hepatitis B viral infection in adults: A systematic review and meta-analysis. Hepatology. 2016;63:284-306.[PubMed Abstract] -
- 16.Ghany MG. Current treatment guidelines of chronic hepatitis B: The role of nucleos(t)ide analogues and peginterferon. Best Pract Res Clin Gastroenterol. 2017;31:299-309.[PubMed Abstract] -
- 17.Li Y, Huang YS, Wang ZZ, et al. Systematic review with meta-analysis: the diagnostic accuracy of transient elastography for the staging of liver fibrosis in patients with chronic hepatitis B. Aliment Pharmacol Ther. 2016;43:458-69.[PubMed Abstract] -
- 18.Choong CC, Venkatesh SK, Siew EP. Accuracy of routine clinical ultrasound for staging of liver fibrosis. J Clin Imaging Sci. 2012;2:58.[PubMed Abstract] -
- 19.Lurie Y, Webb M, Cytter-Kuint R, Shteingart S, Lederkremer GZ. Non-invasive diagnosis of liver fibrosis and cirrhosis. World J Gastroenterol. 2015;21:11567-83.[PubMed Abstract] -
- 20.Kim BK, Kim DY, Park JY, et al. Validation of FIB-4 and comparison with other simple noninvasive indices for predicting liver fibrosis and cirrhosis in hepatitis B virus-infected patients. Liver Int. 2010;30:546-53.[PubMed Abstract] -
- 21.Li J, Gordon SC, Rupp LB, et al. The validity of serum markers for fibrosis staging in chronic hepatitis B and C. J Viral Hepat. 2014;21:930-7.[PubMed Abstract] -
- 22.Keeffe EB, Dieterich DT, Han SH, et al. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: 2008 update. Clin Gastroenterol Hepatol. 2008;6:1315-41.[PubMed Abstract] -
- 23.Lok AS, Heathcote EJ, Hoofnagle JH. Management of hepatitis B: 2000--summary of a workshop. Gastroenterology. 2001;120:1828-53.[PubMed Abstract] -
- 24.Chen CJ, Yang HI, Su J, et al. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA. 2006;295:65-73.[PubMed Abstract] -
- 25.Iloeje UH, Yang HI, Su J, Jen CL, You SL, Chen CJ. Predicting cirrhosis risk based on the level of circulating hepatitis B viral load. Gastroenterology. 2006;130:678-86.[PubMed Abstract] -
- 26.Terrault NA, Bzowej NH, Chang KM, Hwang JP, Jonas MM, Murad MH. AASLD guidelines for treatment of chronic hepatitis B. Hepatology. 2016;63:261-83.[PubMed Abstract] -
- 27.Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology. 2007;45:507-39.[PubMed Abstract] -
- 28.Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med. 2002;137:1-10.[PubMed Abstract] -
- 29.Kariv R, Leshno M, Beth-Or A, et al. Re-evaluation of serum alanine aminotransferase upper normal limit and its modulating factors in a large-scale population study. Liver Int. 2006;26:445-50.[PubMed Abstract] -
- 30.Hoofnagle JH, Doo E, Liang TJ, Fleischer R, Lok AS. Management of hepatitis B: summary of a clinical research workshop. Hepatology. 2007;45:1056-75.[PubMed Abstract] -
- 31.McMahon BJ. Natural history of chronic hepatitis B. Clin Liver Dis. 2010;14:381-96.[PubMed Abstract] -
- 32.McMahon BJ. The natural history of chronic hepatitis B virus infection. Hepatology. 2009;49:S45-55.[PubMed Abstract] -
- 33.Sorrell MF, Belongia EA, Costa J, et al. National Institutes of Health Consensus Development Conference Statement: management of hepatitis B. Ann Intern Med. 2009;150:104-10.[PubMed Abstract] -
- 34.Tseng TC, Kao JH. Treating Immune-tolerant Hepatitis B. J Viral Hepat. 2015;22:77-84.[PubMed Abstract] -
- 35.Chen CJ, Yang HI. Natural history of chronic hepatitis B REVEALed. J Gastroenterol Hepatol. 2011;26:628-38.[PubMed Abstract] -
- 36.Lai M, Hyatt BJ, Nasser I, Curry M, Afdhal NH. The clinical significance of persistently normal ALT in chronic hepatitis B infection. J Hepatol. 2007;47:760-7.[PubMed Abstract] -
- 37.Chen JD, Yang HI, Iloeje UH, et al. Carriers of inactive hepatitis B virus are still at risk for hepatocellular carcinoma and liver-related death. Gastroenterology. 2010;138:1747-54.[PubMed Abstract] -
- 38.Tang AS, Thornton K, and HBV Primary Care Workgroup. Hepatitis B Management: Guidance for the Primary Care Provider. February 25, 2020.
- 39.Brown RS Jr, McMahon BJ, Lok AS, et al. Antiviral therapy in chronic hepatitis B viral infection during pregnancy: A systematic review and meta-analysis. Hepatology. 2016;63:319-33.[PubMed Abstract] -
- 40.Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. Department of Health and Human Services. Initiation of antiretroviral therapy. December 18, 2019.[HIV.gov] -
- 41.Panel on Opportunistic Infections in Adults and Adolescents with HIV. Guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV: recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. Hepatitis B virus infection. Last Updated: December 16, 2024.[HIV.gov] -
- 42.Falade-Nwulia O, Seaberg EC, Rinaldo CR, Badri S, Witt M, Thio CL. Comparative risk of liver-related mortality from chronic hepatitis B versus chronic hepatitis C virus infection. Clin Infect Dis. 2012;55:507-13.[PubMed Abstract] -
- 43.Thio CL, Seaberg EC, Skolasky R Jr, et al. HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter Cohort Study (MACS). Lancet. 2002;360:1921-6.[PubMed Abstract] -
- 44.Perrillo RP, Gish R, Falck-Ytter YT. American Gastroenterological Association Institute technical review on prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology. 2015;148:221-244.e3.[PubMed Abstract] -
- 45.Blackard JT, Sherman KE. Hepatitis B virus (HBV) reactivation-The potential role of direct-acting agents for hepatitis C virus (HCV). Rev Med Virol. 2018;28:e1984.[PubMed Abstract] -
- 46.Mücke MM, Backus LI, Mücke VT, et al. Hepatitis B virus reactivation during direct-acting antiviral therapy for hepatitis C: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2018;3:172-180.[PubMed Abstract] -
- 47.Hare CB, et al. The phase 3 Discover Study: Daily F/TAF or F/TDF for HIV Preexposure Prophylaxis. Abstract 104LB. Presented at: Conference on Retroviruses and Opportunistic Infections; March 4-7, 2019; Seattle.[CROI] -
- 48.US Public Health Service. Preexposure prophylaxis for the prevention of HIV infection in the United States—2017 Update. March 2018:1-77.[CDC] -
Additional References
- Ahn J, Lee HM, Lim JK, et al. Entecavir safety and effectiveness in a national cohort of treatment-naïve chronic hepatitis B patients in the US - the ENUMERATE study. Aliment Pharmacol Ther. 2016;43:134-44.[PubMed Abstract] -
- Ahn J, Lim JK, Lee HM, et al. Lower Observed Hepatocellular Carcinoma Incidence in Chronic Hepatitis B Patients Treated With Entecavir: Results of the ENUMERATE Study. Am J Gastroenterol. 2016;111:1297-304.[PubMed Abstract] -
- Baqai S, Proudfoot J, Xu R, Kane S, Clark M, Gish R. Comparable efficacy with entecavir monotherapy and tenofovir-entecavir combination in chronic hepatitis B patients. BMJ Open Gastroenterol. 2015;2:e000030.[PubMed Abstract] -
- Chang TT, Gish RG, de Man R, et al. A comparison of entecavir and lamivudine for HBeAg-positive chronic hepatitis B. N Engl J Med. 2006;354:1001-10.[PubMed Abstract] -
- Chang TT, Gish RG, Hadziyannis SJ, et al. A dose-ranging study of the efficacy and tolerability of entecavir in lamivudine-refractory chronic hepatitis B patients. Gastroenterology. 2005;129:1198-1209.[PubMed Abstract] -
- Chang TT, Lai CL, Kew Yoon S, et al. Entecavir treatment for up to 5 years in patients with hepatitis B e antigen-positive chronic hepatitis B. Hepatology. 2010;51:422-30.[PubMed Abstract] -
- Chang TT, Liaw YF, Wu SS, et al. Long-term entecavir therapy results in the reversal of fibrosis/cirrhosis and continued histological improvement in patients with chronic hepatitis B. Hepatology. 2010;52:886-93.[PubMed Abstract] -
- Chen G, Lin W, Shen F, Iloeje UH, London WT, Evans AA. Past HBV viral load as predictor of mortality and morbidity from HCC and chronic liver disease in a prospective study. Am J Gastroenterol. 2006;101:1797-803.[PubMed Abstract] -
- Cohen C, Holmberg SD, McMahon BJ, et al. Is chronic hepatitis B being undertreated in the United States? J Viral Hepat. 2011;18:377-83.[PubMed Abstract] -
- Colli A, Fraquelli M, Andreoletti M, Marino B, Zuccoli E, Conte D. Severe liver fibrosis or cirrhosis: accuracy of US for detection--analysis of 300 cases. Radiology. 2003;227:89-94.[PubMed Abstract] -
- Di Marco V, Lo Iacono O, Cammà C, et al. The long-term course of chronic hepatitis B. Hepatology. 1999;30:257-64.[PubMed Abstract] -
- Flemming JA, Terrault NA. Tenofovir vs Entecavir for hepatocellular carcinoma prevention in patients with chronic hepatitis B: one of these things Is not like the other. JAMA Oncol. 2019;5:17-18.[PubMed Abstract] -
- Ganem D, Prince AM. Hepatitis B virus infection--natural history and clinical consequences. N Engl J Med. 2004;350:1118-29.[PubMed Abstract] -
- Gish RG, Chang TT, Lai CL, et al. Loss of HBsAg antigen during treatment with entecavir or lamivudine in nucleoside-naïve HBeAg-positive patients with chronic hepatitis B. J Viral Hepat. 2009;17:16-22.[PubMed Abstract] -
- Gish RG, Chang TT, Lai CL, et al. Quantitative hepatitis B surface antigen analysis in hepatitis B e antigen-positive nucleoside-naive patients treated with entecavir. Antivir Ther. 2013;18:691-8.[PubMed Abstract] -
- Gish RG, Lok AS, Chang TT, et al. Entecavir therapy for up to 96 weeks in patients with HBeAg-positive chronic hepatitis B. Gastroenterology. 2007;133:1437-44.[PubMed Abstract] -
- Hosaka T, Suzuki F, Kobayashi M, et al. Long-term entecavir treatment reduces hepatocellular carcinoma incidence in patients with hepatitis B virus infection. Hepatology. 2013;58:98-107.[PubMed Abstract] -
- Katz LH, Fraser A, Gafter-Gvili A, Leibovici L, Tur-Kaspa R. Lamivudine prevents reactivation of hepatitis B and reduces mortality in immunosuppressed patients: systematic review and meta-analysis. J Viral Hepat. 2008;15:89-102.[PubMed Abstract] -
- Kim GA, Lim YS, Han S, et al. High risk of hepatocellular carcinoma and death in patients with immune-tolerant-phase chronic hepatitis B. Gut. 2018;67:945-52.[PubMed Abstract] -
- Liaw YF, Sung JJ, Chow WC, et al. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med. 2004;351:1521-31.[PubMed Abstract] -
- Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology. 2009;50:661-2.[PubMed Abstract] -
- Lok AS, Zoulim F, Dusheiko G, Ghany MG. Hepatitis B cure: From discovery to regulatory approval. Hepatology. 2017;66:1296-1313.[PubMed Abstract] -
- Marcellin P, Gane E, Buti M, et al. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open-label follow-up study. Lancet. 2013;381:468-75.[PubMed Abstract] -
- Martin P, Lau DT, Nguyen MH, et al. A Treatment Algorithm for the Management of Chronic Hepatitis B Virus Infection in the United States: 2015 Update. Clin Gastroenterol Hepatol. 2015;13:2071-87.e16.[PubMed Abstract] -
- Nana J, Skaare K, Bosson JL, et al. EASL-ALEH 2015 algorithm for the use of transient elastography in treatment-naive patients with hepatitis B: An independent validation. J Viral Hepat. 2021;28:1169-76.[PubMed Abstract] -
- Niederau C, Heintges T, Lange S, et al. Long-term follow-up of HBeAg-positive patients treated with interferon alfa for chronic hepatitis B. N Engl J Med. 1996;334:1422-7.[PubMed Abstract] -
- Seto WK, Lo YR, Pawlotsky JM, Yuen MF. Chronic hepatitis B virus infection. Lancet. 2018;392:2313-24.[PubMed Abstract] -
- Shamliyan TA, MacDonald R, Shaukat A, et al. Antiviral therapy for adults with chronic hepatitis B: a systematic review for a National Institutes of Health Consensus Development Conference. Ann Intern Med. 2009;150:111-24.[PubMed Abstract] -
- Sinn DH, Kim SE, Kim BK, Kim JH, Choi MS. The risk of hepatocellular carcinoma among chronic hepatitis B virus-infected patients outside current treatment criteria. J Viral Hepat. 2019 Jul 22. [Epub ahead of print][PubMed Abstract] -
- Tang B, Kruger WD, Chen G, et al. Hepatitis B viremia is associated with increased risk of hepatocellular carcinoma in chronic carriers. J Med Virol. 2004;72:35-40.[PubMed Abstract] -
- Yao FY, Bass NM. Lamivudine treatment in patients with severely decompensated cirrhosis due to replicating hepatitis B infection. J Hepatol. 2000;33:301-7.[PubMed Abstract] -
Figures
 Figure 1. Baseline HBV DNA Levels and Risk of Developing Hepatocellular CarcinomaSource: Chen CJ, Yang HI, Su J, et al. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA. 2006;295:65-73.
Figure 1. Baseline HBV DNA Levels and Risk of Developing Hepatocellular CarcinomaSource: Chen CJ, Yang HI, Su J, et al. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA. 2006;295:65-73. Figure 2. Baseline HBV DNA Levels and Risk of Developing CirrhosisThese data are from persons with chronic HBV infection who have a negative anti-hepatitis C virus antibody test. This graphic shows a clear correlation of HBV DNA levels and risk of developing cirrhosis.Source: Iloeje UH, Yang HI, Su J, Jen CL, You SL, Chen CJ. Predicting cirrhosis risk based on the level of circulating hepatitis B viral load. Gastroenterology. 2006;130:678-86.
Figure 2. Baseline HBV DNA Levels and Risk of Developing CirrhosisThese data are from persons with chronic HBV infection who have a negative anti-hepatitis C virus antibody test. This graphic shows a clear correlation of HBV DNA levels and risk of developing cirrhosis.Source: Iloeje UH, Yang HI, Su J, Jen CL, You SL, Chen CJ. Predicting cirrhosis risk based on the level of circulating hepatitis B viral load. Gastroenterology. 2006;130:678-86. Figure 3. Hepatitis B Disease PhasesThis illustrations shows relationship of different hepatitis B immune phases and fluctuations in HBV DNA and serum alanine aminotransferase (ALT) levels.Illustration: David H. Spach, MD
Figure 3. Hepatitis B Disease PhasesThis illustrations shows relationship of different hepatitis B immune phases and fluctuations in HBV DNA and serum alanine aminotransferase (ALT) levels.Illustration: David H. Spach, MDTables
Table 1. HBV Treatment Recommendation Based on Major Organization Guidelines
Risk Group AASLD
2018APASL
2015EASL
2017WHO
2024Without cirrhosis
Treat if:
- ALT ≥2x ULN1, or
- Significant histologic disease2
and
- HBV DNA >2000 IU/mL if HBeAg-negative
- HBV DNA >20,000 IU/mL if HBeAg-positiveTreat if:
- ALT >2x ULN3, or
- Significant histologic disease3
and
- HBV DNA >2000 IU/mL if HBeAg-negative
- HBV DNA >20,000 IU/mL if HBeAg-positiveTreat if:
- ALT >40 IU/L, HBV DNA >2,000 IU/mL, and biopsy evidence of at least moderate necroinflammation or fibrosis, or
- HBV DNA >2,000 IU/mL and biopsy evidence of at least moderate fibrosis, or
- HBV DNA >20,000 IU/mL and ALT > 2x ULN3 regardless of degree of fibrosisTreat if any:
- Significant fibrosis5
- Coinfection with HCV, HDV, or HIV
- Family history of liver cancer or cirrhosis
- Comorbidities
- Immune suppression
- Extrahepatic
- Persistent abnormal ALT6Compensated cirrhosis
Treat all4
Treat if:
- HBV DNA >2,000 IU/mL, or
- ALT elevated3Treat all4
Treat all4 Decompensated cirrhosis
Treat all4 and refer for liver transplantation Treat all4 Treat all4 Treat all4
Abbreviations: ASLD = American Association for the Study of Liver Diseases; APASL = Asian Pacific Association for the Study of the Liver; EASL= European Association for the Study of the Liver; WHO = World Health Organization; ALT = alanine aminotransferase; ULN = upper limit of normal
1Regardless of HBV DNA, ALT, or HBeAg status; 2Upper limit of normal, defined as ALT 35 IU/L for men, 25 IU/L for women; 3Defined as ALT 40 IU/L for both men and women; 4Defined as at least moderate necroinflammation or at least moderate fibrosis according to histopathologic grading/staging; 5The thresholds for significant fibrosis by APRI or transient elastography have not been fully validated in adolescents; 6Defined as two ALT values greater than 19 IU/L for women and 39 IU/L for men at unspecified intervals during a 6- to 12-month period.Source:- European Association For The Study Of The Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67:370-98. [PubMed Abstract]
- Sarin SK, Kumar M, Lau GK, et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 update. Hepatol Int. 2016;10:1-98. [PubMed Abstract]
- Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67:1560-99. [PubMed Abstract]
- World Health Organization. Guidelines for the prevention, diagnosis, care and treatment for people with chronic hepatitis B infection. March 29, 2024. [WHO]
- Lesson 2







Since you've received 80% or better on this quiz, you may claim continuing education credit.
You seem to have a popup blocker enabled. If you want to skip this dialog please Always allow popup windows for the online course.