Lesson 3. HBV Immunizations
Associate Editor
Associate Professor of Medicine
Division of Allergy & Infectious Diseases
University of Washington
Editor-in-Chief
Professor of Medicine
Division of Allergy & Infectious Diseases
University of Washington
Associate Editor
Professor of Medicine
Division of Allergy & Infectious Diseases
University of Washington
Learning Objective Performance Indicators
- Implement hepatitis B virus (HBV) vaccination as a core intervention to prevent and eliminate HBV infection
- Identify populations that should receive HBV vaccination
- Summarize rationale for HBV pre- and postvaccination serologic testing
- Use appropriate dosing, scheduling, and administration of single-antigen or combination vaccines in children and adults
- Initiate strategies to manage HBV vaccine nonresponders
Background
Vaccination is the mainstay of hepatitis B virus (HBV) prevention and represents a core intervention in the World Health Organization’s (WHO) efforts to eliminate hepatitis B by 2030.[1] Following the licensure of the first hepatitis B vaccine in 1981, there have been major advances in hepatitis B vaccines. In addition, vaccine recommendations have evolved over the past several decades, culminating in the recommendation for universal hepatitis B immunization for all persons younger than 60 years of age.[2] The following briefly summarizes the chronology and type of hepatitis B vaccines licensed for use in the United States (Figure 1).
- The first hepatitis B vaccine, which was plasma-derived, was licensed in the United States in 1981.[3] This vaccine contained purified plasma-derived hepatitis B surface antigen (HBsAg) and was safe and highly successful in preventing HBV infection.[3,4,5] Nevertheless, the first-generation plasma-derived HBV vaccine was tedious to manufacture, and the plasma-derived vaccine led to unsubstantiated concerns regarding the potential for bloodborne pathogen transmission and was eventually discontinued in 1992.[3]
- By the mid-1980s, the second generation of hepatitis B vaccines became commercially available—Recombivax-HB and Engerix-B. These vaccines utilized recombinant DNA technology to express a nonglycosylated hepatitis B surface antigen in yeast cells, a process that was more cost-effective and scalable than the plasma-derived method.[3,4] Furthermore, yeast-derived vaccines eliminate any concern for vaccine-related bloodborne pathogen transmission.[3]
- In the 1990s, mammalian cell-derived HBV vaccines became commercially available. These vaccines contained both the S antigen and either the pre-S2 or the pre-S2 and pre-S1 HBV antigens. Although studies suggested these vaccines were efficacious in conventional HBV vaccine nonresponders and overall more immunogenic than yeast-derived recombinant vaccines, manufacturing costs were higher, and they were not widely used.[6]
- In 2017, the hepatitis B vaccine, Heplisav-B, was approved by the Food and Drug Administration (FDA). Heplisav-B contains a yeast-derived recombinant HBsAg as well as a novel cytidine-phosphate-guanosine oligodeoxynucleotide (CpG ODN) adjuvant that binds toll-like receptor 9 and stimulates a more robust immune response to HBsAg than the historical alum adjuvant.[7] The Heplisav B vaccine is recommended for use in adults 18 years of age and older and represents the fifth inactivated HBV vaccine recommended in the United States.[7]
Vaccine Uptake
Hepatitis B Vaccine Coverage Among Adults
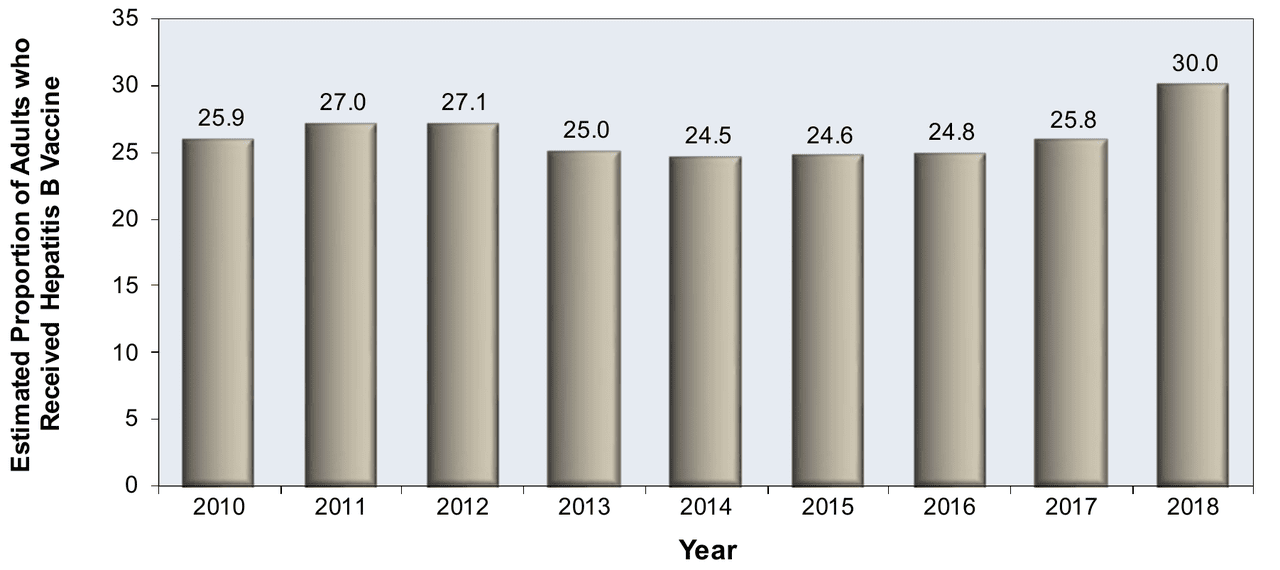
Although acceptance is high among adults who are offered hepatitis B vaccination, the overall hepatitis B vaccine coverage is low in the adult population. The National Health Interview Survey (NHIS) survey conducted during August 2017–June 2018 estimated hepatitis B vaccine coverage was 30% for adults 19 years of age and older during the year 2018.[8] In this survey, the vaccine coverage varied by age: younger adults 19–49 years of age had a 40% hepatitis B vaccine coverage rate compared with only 19% for those 50 years of age and older.[8] From 2010-2018, hepatitis B vaccine coverage among adults 19 years of age and older increased (range 24.5%-30.0%) (Figure 2).[8] In an earlier survey of men who have sex with men (MSM) surveyed in the Young Men's Health Study, only 17% had received a hepatitis B vaccine series, despite more than 90% of HBV-susceptible MSM in this study reporting access to health care services, including testing for HIV and other sexually transmitted infections.[9] The low rate of HBV immunization in these instances represents missed opportunities to provide hepatitis B immunization to adults and highlights the need for increased HBV education in primary care regarding recent simplified universal vaccination guidance.[2]
Hepatitis B Vaccine Coverage Among Children
Among children, hepatitis B vaccine coverage is better, with an estimated 91.1% of children born between 2020 and 2021 receiving at least 3 doses of the hepatitis B vaccine by age 24 months.[10] Similarly, in 2023, an estimated 90.9% of U.S. adolescents aged 13–17 years received at least 3 doses of the hepatitis B vaccine.[11] Nevertheless, despite these relatively high numbers, these estimates for infant and adolescent vaccine coverage are down slightly from prior years, a finding that may reflect growing vaccine hesitancy and/or disruptions in routine vaccination owing to the COVID-19 pandemic.[10,11]
Indications for Hepatitis B Vaccination
Historical Hepatitis B Recommendations in the United States
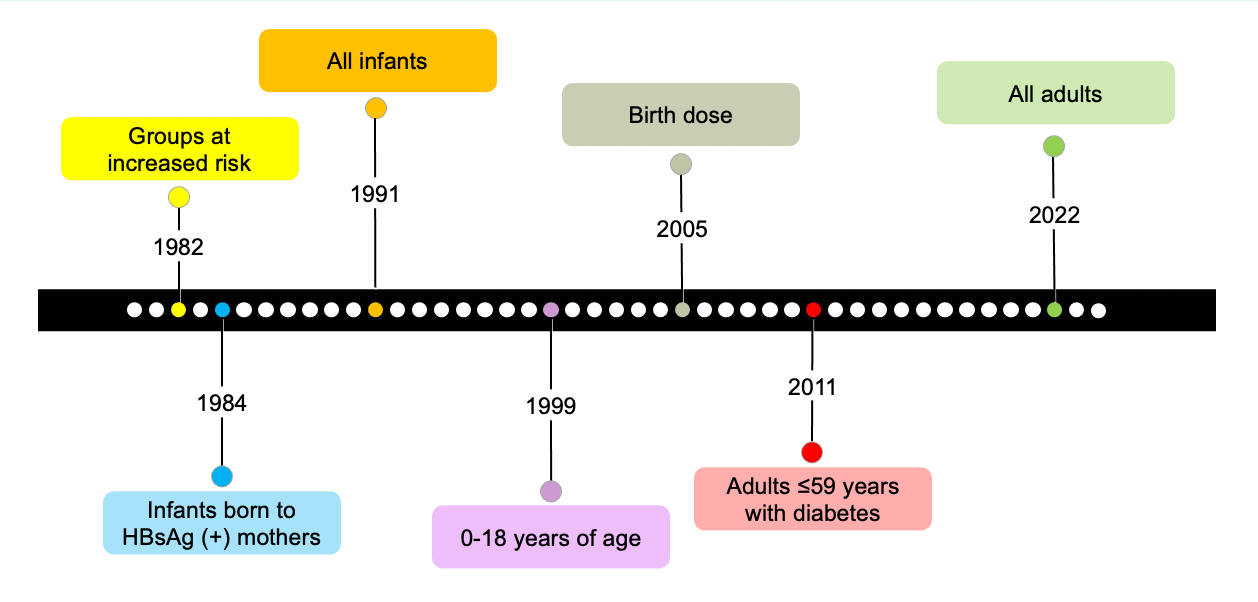
Beginning in 1982, the Centers for Disease Control (CDC) and the Advisory Committee on Immunization Practices (ACIP) issued recommendations for hepatitis B vaccination for groups at risk of acquiring HBV, with recommendations subsequently expanding incrementally to include more groups for whom routine hepatitis B vaccine is indicated (Figure 3).[2,12,13,14,15,16]
Universal Hepatitis B Vaccine Recommendations
In 2022, the ACIP issued updated recommendations for hepatitis B vaccinations that called for universal hepatitis B vaccination in adults aged 19–59 years of age.[2] Based on these new recommendations, in the United States, hepatitis B vaccination is now recommended for all infants, all unvaccinated children and adolescents younger than age 19, and all unvaccinated adults 19 to 59 years of age.[2] In addition, hepatitis B vaccination is recommended for adults 60 years of age and older with risk factors for HBV acquisition.[2] The table below summarizes the most recent and current ACIP hepatitis B vaccine recommendations, and the text following the table provides some additional details on each of the categories (Table 1).[2]
- All Infants: All infants should receive the hepatitis B vaccine series as part of the routine childhood immunization schedule. The number of hepatitis B vaccine doses and the exact timing of vaccination differ slightly depending on the infant’s birth weight, the maternal HBsAg status, and the vaccine used. For more detailed information, see Preventing HBV Perinatal Transmission.
- Unvaccinated Children Younger than 19 Years of Age: Children and adolescents who have not previously received the hepatitis B vaccine should be vaccinated as part of routine “catch-up vaccination,” regardless of age.
- Adults 19 to 59 Years of Age: All adults 19 to 59 years of age should receive the hepatitis B vaccine. Adults who previously completed a hepatitis B vaccine series do not need additional hepatitis B vaccination. Persons with a history of HBV infection and those with active hepatitis B infection should not receive hepatitis B vaccination.
- Adults 60 years of Age and Older with Risk Factors for Hepatitis B: Adults 60 years of age and older, who have not completed the hepatitis B vaccine series and have no history of HBV infection, should be vaccinated against HBV if they are among any of the following groups:
- Persons at Risk for HBV Infection by Sexual Exposure: Sexual exposure is a well-defined risk factor for HBV acquisition and is likely responsible for more than 30% of incident HBV infections in the United States.[17] The following summarizes groups that should receive hepatitis B vaccination due to the risk of HBV acquisition from sexual exposure:
- Sex partners of HBsAg-positive persons
- Sexually active persons who are not in a long-term, mutually monogamous relationship (e.g., persons with more than one sex partner during the previous 6 months)
- Persons seeking evaluation or treatment for a sexually transmitted infection
- Men who have sex with men
- Persons at Risk for Infection by Percutaneous Exposure: Percutaneous exposure is one of the most common risk factors for HBV acquisition in the United States, mainly due to the recent rise in injection drug use.[17,18,19] There are, however, several other groups, including health care workers, persons in long-term care facilities, and persons living with someone known to be HBsAg-positive, also known to be at risk for HBV via percutaneous exposure. The following summarizes persons who should receive the hepatitis B vaccine due to the risk of percutaneous or mucosal exposure:
- Persons who currently or recently injected drugs
- Household contacts of HBsAg-positive persons
- Residents and staff of facilities for persons with developmental disabilities
- Health care and public safety personnel with reasonably anticipated risk of exposure to blood or blood-contaminated body fluids
- Persons receiving hemodialysis, predialysis, peritoneal dialysis, or home dialysis
- Persons with diabetes 60 years of age and older, at the discretion of the treating clinician
- Persons at Risk for HBV Infection by Sexual Exposure: Sexual exposure is a well-defined risk factor for HBV acquisition and is likely responsible for more than 30% of incident HBV infections in the United States.[17] The following summarizes groups that should receive hepatitis B vaccination due to the risk of HBV acquisition from sexual exposure:
- Others at Increased Risk of Acquiring HBV Infection
- International travelers to countries with low-intermediate to high levels of endemic HBV infection, as defined by an HBsAg prevalence of 2% or greater (see the lesson HBV Epidemiology for CDC country prevalence estimates)
- Persons with hepatitis C virus infection
- Persons with chronic liver disease (including, but not limited to, persons with cirrhosis, fatty liver disease, alcohol-associated liver disease, autoimmune hepatitis, and an alanine aminotransferase [ALT] or aspartate aminotransferase [AST] level greater than twice the upper limit of normal)
- Persons with HIV infection
- Incarcerated persons
- Adults 60 Years of Age and Older without Risk Factors: Adults 60 years of age and older without known risk factors for HBV may receive the hepatitis B vaccine.
Prevaccination Serologic Testing
Potential Role of Prevaccination Serologic Testing
Prevaccination serologic testing has two potential roles: to identify persons with existing immunity to HBV who do not require vaccination and to detect persons with chronic active HBV.[15] If hepatitis B vaccination is administered to persons who are already immune to HBV (or chronically infected with HBV), it does not increase the risk for vaccine-related adverse events.[14]In general, routine prevaccination serologic testing is not recommended in settings where background immunity to hepatitis B is low, as it is not cost-effective.[15,20,21,22] In populations with a high HBsAg prevalence or with a high risk for chronic HBV, prevaccination serologic testing may reduce costs by avoiding unnecessary vaccinations. In these settings, prevaccination serologic testing also offers the opportunity to identify persons with chronic HBV infection and link them to care for management of chronic HBV infection.[2]
Persons Recommended for Prevaccination Serologic Testing
Prevaccination serologic screening for hepatitis B should include the groups listed below, but note that lack of access to prevaccination testing should not be a barrier to vaccination.[2,15]
- Household, sexual, or needle contacts of HBsAg–positive persons
- Persons with HIV infection
- Persons with elevated alanine aminotransferase/aspartate aminotransferase of unknown etiology
- Hemodialysis patients
- Men who have sex with men
- Persons who inject drugs (past or present)
- Persons born in countries of low-intermediate to high HBV endemicity (HBsAg prevalence ≥2%)
- United States-born persons not vaccinated as infants whose parents were born in countries with high HBV endemicity (≥8%)
- Persons needing immunosuppressive therapy, including chemotherapy, immunosuppression related to organ transplantation, and immunosuppression for rheumatologic or gastroenterologic disorders
- Donors of blood, plasma, organs, tissues, or semen
Recommended Prevaccination Serologic Tests
If hepatitis B prevaccination serologic testing is performed, the CDC guidance recommends obtaining the following tests:[2,15]
- Hepatitis B surface antigen (HBsAg), and
- Antibody to HBsAg (anti-HBs), and
- Antibody to hepatitis B core antigen (anti-HBc).
Serologic Testing and Timing of Hepatitis B Vaccination
Prevaccination serologic testing should not be a barrier to vaccination of persons potentially susceptible to HBV infection, especially hard-to-reach populations.[2,15] If prevaccination serologic testing is indicated, the first dose of hepatitis B vaccine can be delivered at the time blood is collected for serologic testing; if the serologic testing shows the person is immune or has HBV infection, then no further doses of the vaccine should be given. In venues where hepatitis B vaccination is recommended and serologic testing is not feasible, hepatitis B vaccination should simply be provided.[2,14,15,23]
HBV Vaccines and Schedules
HBV Vaccines Approved for Use in the United States
There are currently three single-antigen hepatitis B vaccines approved for use in the United States: Engerix-B, Recombivax HB, and Heplisav-B.[7,15] There are three FDA-approved combination vaccines that provide hepatitis B immunization in conjunction with other antigens; these include Twinrix (hepatitis A and B combination vaccine), Pediarix (combination vaccine containing hepatitis B, diphtheria-tetanus-acellular pertussis [DTaP]), and inactivated poliovirus), and Vaxelis (hepatitis B, DTaP, inactivated poliovirus, and Haemophilus influenzae).[15] The following table summarizes the dose and volume administered with each of these vaccines for all age groups, persons receiving hemodialysis, and immunocompromised individuals; the amount of HBsAg and volume administered with each vaccine dose varies significantly based on age, which vaccine is used, and whether the individual is receiving hemodialysis.[2,7,15]
| Single-Antigen Vaccines | Combination Vaccines | |||||||||||
| Age group (years) | Recombivax-HB | Engerix-B | Heplisav-B^ | Pediarix* | Twinrix† | |||||||
| Dose (µg) |
Vol (mL) |
Dose (µg) |
Vol (mL) |
Dose (µg) |
Vol (mL) |
Dose (µg) |
Vol (mL) |
Dose (µg) |
Volume (mL) |
|||
| Standard Dosing | ||||||||||||
| Birth-10 | 5 | 0.5 | 10 | 0.5 | N/A | N/A | 10* | 0.5 | N/A | N/A | ||
| 11-15 | 10§ | 1.0 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | ||
| 11-19 | 5 | 0.5 | 10 | 0.5 | N/A | N/A | N/A | N/A | N/A | N/A | ||
| ≥20 | 10 | 1.0 | 20 | 1.0 | 20 | 0.5 | N/A | N/A | 20† | 1.0 | ||
| Dosing in Hemodialysis Patients and Other Immunocompromised Persons | ||||||||||||
| <20 | 5 | 0.5 | 10 | 0.5 | N/A | N/A | N/A | N/A | N/A | N/A | ||
| ≥20 | 40# | 1.0# | 40 | 2.0 | N/A | N/A | N/A | N/A | N/A | N/A | ||
|
+Note: this table is modified from original to include information on Heplisav-B |
||||||||||||
- Schillie S, Vellozzi C, Reingold A, et al. Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2018;67:1-31. [PubMed Abstract]
Single-Antigen Vaccines
- Engerix-B: This single-antigen hepatitis B vaccine contains yeast-derived (recombinant) HBsAg combined with an aluminum adjuvant. It is FDA-approved for use in individuals of all ages.
- Heplisav-B: This single-antigen hepatitis B recombinant vaccine consists of recombinant HBsAg combined with the synthetic immunostimulatory cytidine-phosphate-guanosine (CpG) oligodeoxynucleotide 1018 adjuvant; the CpG adjuvant binds to Toll-like receptor 9, signaling an innate immune system pathway in response to the HBsAg antigen. This vaccine is FDA-approved as a 2-dose series for use in persons 18 years of age and older.
- Recombivax-HB: This single-antigen hepatitis B vaccine contains recombinant HBsAg that is also produced in yeast cells and is combined with an aluminum adjuvant; this vaccine is FDA-approved for use in individuals of all ages.
Combination Vaccines
- Twinrix: This bivalent vaccine contains inactivated hepatitis A virus and recombinant HBsAg. Each 1 mL dose contains a lower quantity (720 ELISA units) of hepatitis A vaccine than the standard 1 mL single-antigen hepatitis A vaccine (1440 ELISA units). This vaccine is FDA-approved for use only in persons 18 years of age and older.
- Pediarix: This combination vaccine contains diphtheria toxoid, tetanus toxoid, acellular pertussis antigens, recombinant HBsAg, and inactivated poliovirus. Pediarix is FDA-approved as a 3-dose series in infants born to HBsAg-negative mothers; this vaccine may be given as early as 6 weeks of age and through 6 years of age (prior to the seventh birthday). It is not approved for children younger than 6 weeks of life and thus should not be given for the birth-dose vaccination.
- Vaxelis: This combination vaccine contains diphtheria toxoid, tetanus toxoid, acellular pertussis antigens, inactivated poliovirus, recombinant HBsAg, and Haemophilus influenzae type b. Vaxelis is FDA-approved as a 3-dose series in children 6 weeks through 4 years of age (prior to the fifth birthday). Although this vaccine is FDA-approved, it is not widely available. Accordingly, it will not be discussed further.
Administration of Hepatitis B Vaccines
All hepatitis B vaccines should be administered as intramuscular (IM) injections, with the deltoid muscle the preferred site for adults, adolescents, and children. For infants less than 1 year of age, the anterolateral thigh should be used for intramuscular injection. Administration of any hepatitis B vaccine in the buttocks or subcutaneously is not recommended, since administration by these routes is associated with lower levels of protective immune response. The hepatitis B vaccine should not be given to any person with a history of a serious allergic response to a prior dose of hepatitis B vaccine, a component of the hepatitis B vaccine, or yeast.
Choice and Schedule of HBV Vaccines in Infants
For infants, only the single-antigen hepatitis B vaccines (Engerix-B or Recombivax-HB) are recommended for the birth dose vaccine.[15] The vaccine schedules for infants depend on birth weight and maternal HBsAg status (Table 3).[7,15] The combination vaccine, Pediarix, which contains vaccine components for hepatitis B, DTaP, and inactivated polio vaccine, is approved starting at 2 months of age up through age 6 years, and this 3-dose series can be used to complete the hepatitis B vaccination after a single-antigen hepatitis B vaccine birth dose is given.[15]
Choice and Schedule of HBV Vaccines for Children and Adolescents
For children and adolescents, there are multiple options for hepatitis B immunization (Figure 4). For adolescents 11 through 15 years of age, a 2-dose hepatitis B vaccine series with Recombivax-HB can be used if the adult-strength doses are administered.[7,13,15] In general, rates of protective immunity are similar across different hepatitis B vaccines in immunocompetent infants, children, and adolescents, and vaccine brands are interchangeable within an immunization series.[15] Due to a lack of data on the interchangeability of acellular pertussis-containing vaccines, the American Academy of Pediatrics recommends vaccines from the same manufacturer be used for the pertussis series.[24] Note that Heplisav-B is not approved for use in persons younger than 18 years of age.
Choice and Schedule of HBV Vaccine in Adults
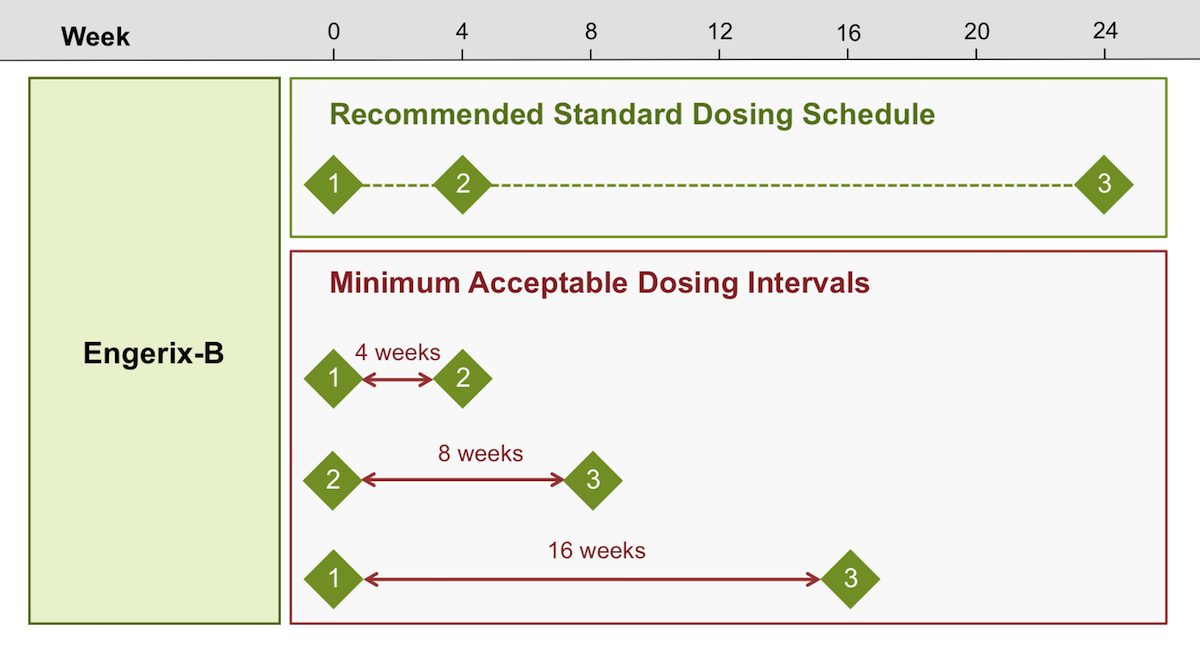
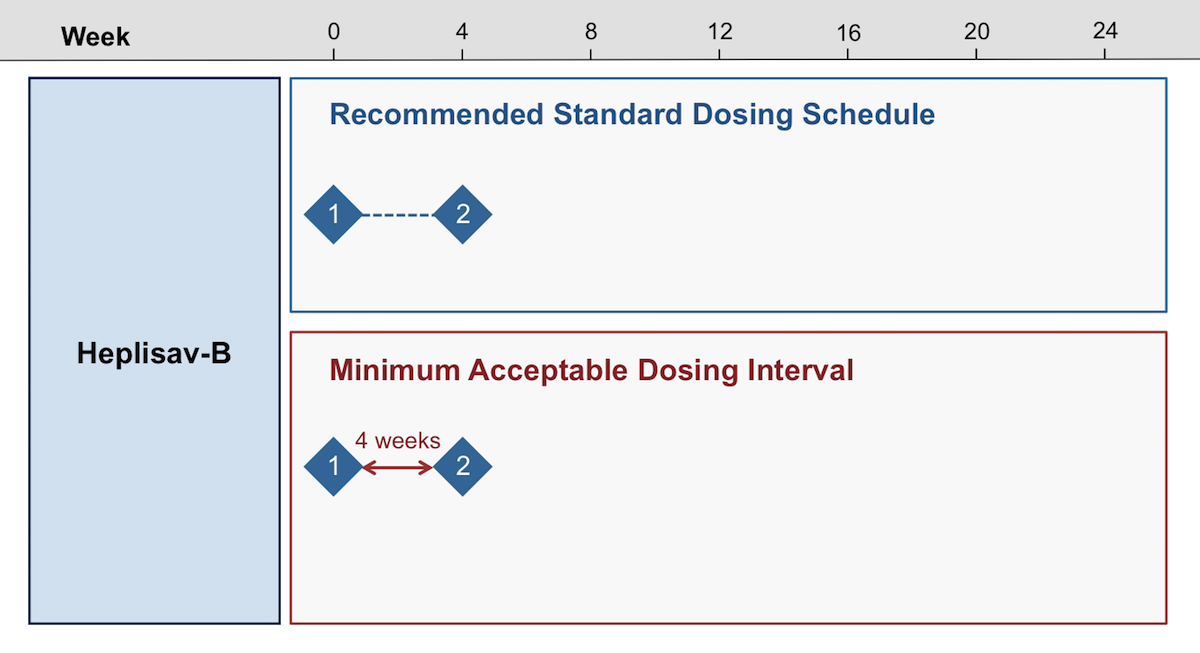
In adults, the ACIP does not preferentially indicate which single-antigen hepatitis B vaccine to use. Nevertheless, many experts now recommend using Heplisav-B in both healthy and immunocompromised adults owing to higher rates of seroprotection and the need for only 2 doses (versus 3 doses with other hepatitis B vaccines). If adults require protection against both hepatitis A virus (HAV) and HBV, then Twinrix (a combination of hepatitis A and hepatitis B vaccines) can be used. The ACIP recommends that the following listed hepatitis B vaccines are safe for administration during pregnancy: Engerix-B, Heplisav-B, Recombivax HB, and Twinrix.[25] In general, the single-antigen hepatitis B vaccines—Engerix-B and Recombivax-HB—can be used interchangeably in adults.[15] For adults, if a 2-dose series is desired, Heplisav-B is the only option, as all other single-antigen vaccines require a three-dose schedule(Figure 5).[7,15]
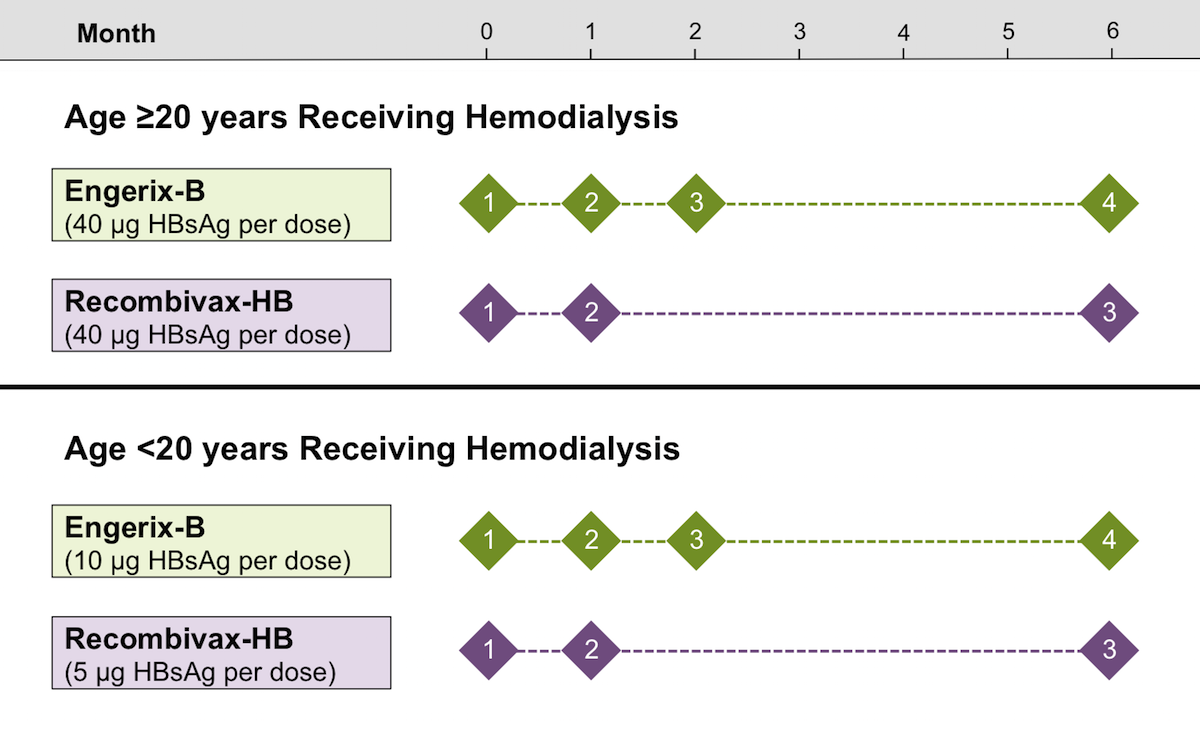
Vaccine Dosing in Persons Receiving Hemodialysis
For persons older than 20 years of age who are receiving hemodialysis, it is important to note that higher doses of Recombivax-HB (40 µg per dose) and Engerix-B (40 µg per dose) are needed due to poor vaccine response rates with standard doses of these vaccines in this population. In addition, when Engerix-B is used for persons on hemodialysis, the usual 3-dose vaccine schedule (0, 1, and 6 months) is expanded to four doses (0, 1, 2, and 6 months) (Figure 6).[15] Persons younger than 20 years of age should receive Recombivax-HB (5 µg per dose) or Engerix-B (10 µg per dose). Although limited data suggest Heplisav-B (a 3-dose schedule with standard dosing) and Twinrix (standard schedule and dosing) may lead to higher rates of HBV seroprotection in hemodialysis patients, there are no specific ACIP recommendations for the use of either of these vaccines in persons receiving hemodialysis.[26,27,28,29]
HBV Immunization in Adults with HIV
For adults with HIV, the two-dose Heplisav-B vaccine is preferentially recommended, given high rates of seroconversion.[30,31] If, however, a recombinant three-dose vaccine (Engerix-B or Recombivax-HB) is used, guidelines recommend administering a double dose (with each dose) for 3 total doses as the primary vaccine series (Figure 7).[30] The recommendation for the use of double-dose vaccine with Engerix-B or Recombivax-HB is based on data from a meta-analysis of 10 studies showing improved response rates at 4 to 6 weeks and at 12 months post-vaccination when double doses are compared to standard doses.[32] For persons with HIV who do not respond to a series with Engerix-B or Recombivax-HB, repeat immunization is recommended, giving 2 or 3 doses of Heplisav-B.[30,33] In addition, a 3-dose series of Twinrix can also be used as an alternative for persons who additionally require vaccination against hepatitis A, but note that each dose of Twinrix is equivalent to only a single-dose strength for hepatitis B antigen.
Interruption in Schedule
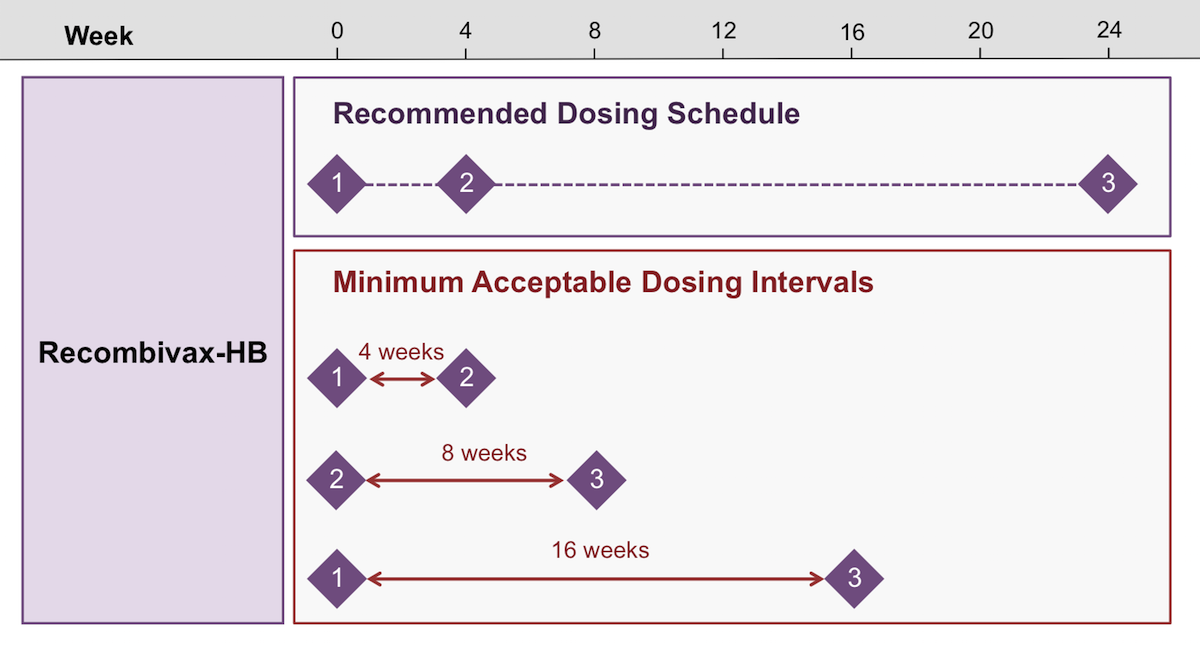
Longer intervals between doses 1 and 2 or doses 2 and 3 of Engerix-B and Recombivax-HB vaccines have not been shown to diminish efficacy, and if anything, a longer than recommended interval between the last two doses of vaccine may confer higher levels of protection.[15] As such, there is no need to restart the hepatitis B vaccine series in situations where the vaccination schedule has been interrupted. Subsequent doses should be given as soon as possible, making sure the first and second doses are separated by at least 4 weeks, the second and third doses are separated by at least 8 weeks, and the third dose is at least 16 weeks after the first dose.[15]
Minimum Acceptable Intervals Between Doses
For Engerix-B, Recombivax-HB, and Heplisav-B, the minimal acceptable dosing interval between the first and second dose of vaccine is 4 weeks (Figure 8).[7,15] The second and third doses of Engerix-B and Recombivax-HB should be given at least 8 weeks apart, and the first and third doses of vaccine should be separated by at least 16 weeks.[7,15] In infants, the third dose of vaccine (Engerix-B, Recombivax-HB, or Pediarix) should not be administered before 24 weeks of age.[15] For all hepatitis B vaccines and all intervals, doses administered up to 4 days before the minimal acceptable dosing intervals are valid; however, doses administered 5 or more days before the minimum dosing interval must be repeated using the correct schedule.[15] The one exception to these dosing intervals is accelerated administration of Twinrix, which can be given in adults at 0, 7, and 21 days, followed by a fourth dose at 12 months.[15] In the case of accelerated Twinrix, the 4-day grace period does not apply.[15]
Response to HBV Vaccines
Response to HBV Vaccines
The overall responses to all hepatitis B vaccines in healthy children and adults have been very good. Lower responses have been seen in persons undergoing hemodialysis and immunocompromised persons, including persons with HIV.
- Engerix B and Recombivax-HB: After three doses of the hepatitis B vaccine, more than 95% of healthy infants and more than 90% of healthy adults younger than 40 years of age achieve protective immunity, defined as an HBsAb level of 10 mIU/mL or greater.[34,35,36] Although it is optimal to administer the complete hepatitis B vaccine series, studies have shown that 32 to 56% of persons can achieve protective levels of anti-hepatitis B surface antibody (HBsAb) with a single dose of Recombivax-HB or Engerix-B, and 70 to 75% achieve protective levels with two doses of vaccine.[34,36]
- Twinrix: In an open-label, randomized, controlled trial of Twinrix versus single-antigen hepatitis A vaccine plus single-antigen hepatitis B vaccine in healthy adults 19 years of age and older, HAV seroconversion and HBV seroprotection occurred in 95.1% of subjects in the Twinrix arm versus 92.2% of subjects in the monovalent vaccine arm.[37]
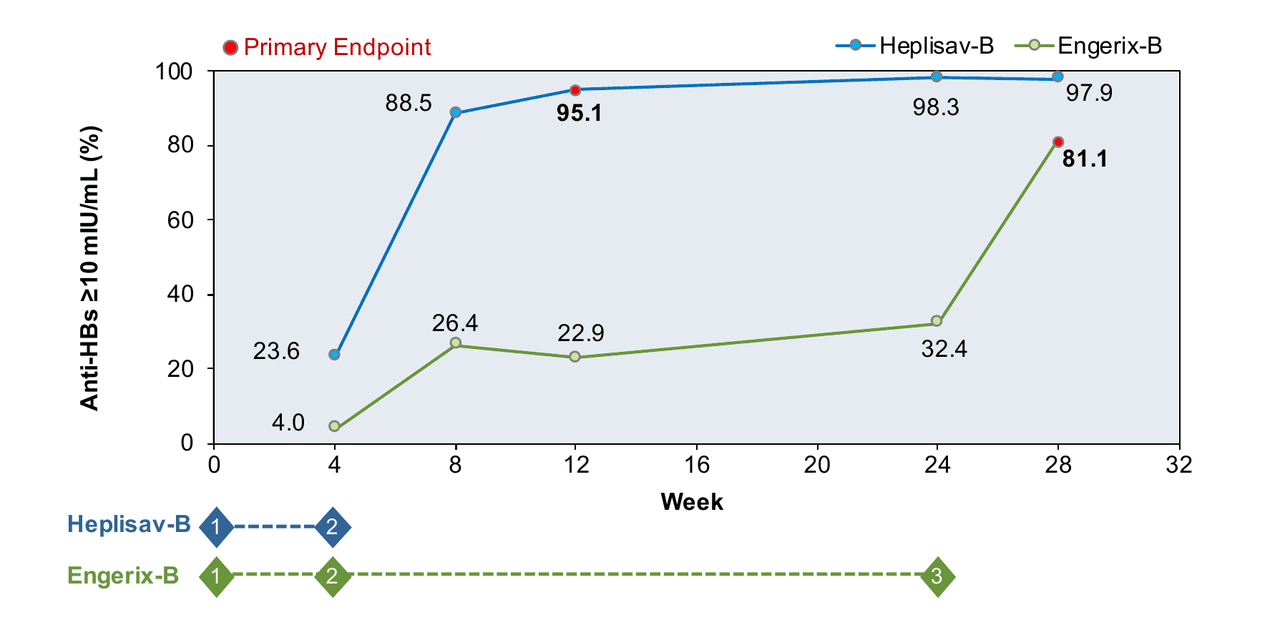
- Heplisav-B: Responses to the two-dose Heplisav-B vaccine are excellent. In phase 3 registration trials that collectively enrolled 9,597 adults aged 18 through 70 years, the seroprotection rate (SPR) after two doses of Heplisav-B, spaced one month apart, was 90 to 100%, compared with 71 to 90% for standard single-antigen hepatitis B vaccine (Engerix-B) for three doses (Figure 9).[38,39,40,41] This improvement in seroconversion rates is particularly notable among groups that have historically had lower seroprotective responses to recombinant hepatitis B vaccines, including persons with older age, diabetes mellitus, tobacco use, obesity, or HIV.[7,31,38,39,42]
Reduced Response to Vaccine
Despite generally high rates of seroconversion in healthy adults, certain conditions are associated with decreased response to hepatitis B vaccines
|
|
|
|
|
|
|
|
|
|
|
- Schillie S, Vellozzi C, Reingold A, et al. Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2018;67:1-31. [PubMed Abstract]
HBV Vaccine in Persons Receiving Hemodialysis
Among persons with chronic kidney disease, the serologic response rates to Engerix-B and Recombivax-HB vaccines (using standard HBsAg doses and standard dosing schedules) are only about 50 to 60%. To improve the vaccine response in adults receiving hemodialysis, each dose of HBsAg in Engerix-B is increased (from 1 mL to 2 mL), and the dosing schedule is expanded from three doses (0, 1, and 6 months) to four doses (0, 1, 2, and 6 months). Similarly, when giving Recombivax-HB to adults receiving hemodialysis, each HBsAg dose is increased from 10 µg to 40 µg, but the same schedule is used (0, 1, and 6 months). In an observer-blind, randomized trial in adults receiving hemodialysis, investigators compared a 3-dose Heplisav-B series (0, 1, and 6 months) with the 4-dose series (0, 1, 2, and 6 months) of double-dose (40 µg) Engerix-B; the seroprotective response rates at weeks 28 and 52 were higher with Heplisav-B than with Engerix-B.[26] Although this study showed promise with a 3-dose Heplisav-B series in persons on hemodialysis, at this time, there are insufficient data on the use of Heplisav-B in persons on hemodialysis.
Duration of Immunity
In general, protection generated by a complete vaccine series is believed to last for at least 30 years in most healthy individuals, and immunity in healthy adults and children appears to persist even though antibodies may decline over time, even below the limit of detection.[49,50,51,52,53] This is evidenced by a study of seroprotection rates in 423 adolescents who received HBV vaccination as infants. In this study, only 24% of participants had protective HBsAb levels of 10 mIU/mL or greater at baseline, but 92% achieved protective levels after a challenge dose of vaccine.[54] A similar study of 243 Alaska Native persons who were vaccinated in infancy showed that 51% had HBsAb levels of 10 mIU/mL or greater after 30 years, and among those with HBsAb levels less than 10 mIU/mL, 88% responded to a booster dose of hepatitis B vaccine, achieving HBsAb levels of 10 mIU/mL or greater.[55] In a subsequent study done within the same Alaska Native population, a group of 112 persons who responded to the initial hepatitis B vaccine series were evaluated 35 years later, and 47% had HBsAb levels of 10 mIU/mL or greater; among those with HBsAb levels less than 10 mIU/mL, 74% responded to a booster dose of hepatitis B vaccine, achieving HBsAb levels of 10 mIU/mL or greater.[53] Based on the proportion of individuals who had anti-HBs levels of 10 mIU/mL or greater at 35 years after immunization and following one booster dose, the authors concluded that 86% of individuals had serologic evidence of HBV protection 35 years following initial vaccination.[53]
Postvaccination Serologic Testing
Indications for Postvaccination Serologic Testing
Postvaccination testing for levels of HBsAb is not recommended following routine hepatitis B immunization of infants, children, adolescents, or adults.[15] The rationale for this recommendation is that most healthy persons have an excellent response to the hepatitis B vaccine series. In contrast, postvaccination serologic testing should be considered for persons who have known ongoing risk for hepatitis B exposure, known diminished protective response to vaccine, or whose clinical management depends on knowledge of their HBV immune status. The purpose of testing in these situations is to determine the need for revaccination, and in the case of sex partners, the need for additional protective measures.[15] The CDC recommends hepatitis B postvaccination serologic testing to determine vaccine immune response in the following groups:[15]
- Infants born to HBsAg-positive mothers
- Infants born to mothers whose HBsAg status remains unknown
- Health care workers and public safety workers who are at risk of continued exposure to blood and body fluids
- Hemodialysis patients and others who might require outpatient hemodialysis (e.g., predialysis, peritoneal dialysis, and home dialysis)
- Persons with HIV and other immunocompromised persons (e.g., hematopoietic stem-cell transplant recipients or persons receiving chemotherapy)
- Sex partners of HBsAg-positive persons
Timing and Method of Postvaccination Serologic Testing
For persons who have an indication for postvaccination serologic testing, the testing should be performed 1 to 2 months after completion of the hepatitis B vaccine series, regardless of which hepatitis B vaccine was used.[7,15] The goal of postvaccination serologic testing is to assess immunity against HBV; performing a quantitative anti-HBs is the recommended test for this assessment. Of note, serologic testing for infants born to HBsAg-positive mothers (or mother with unknown HBsAg status) should also include testing for HBsAg. These infants should have testing performed 1 to 2 months after completing the hepatitis B vaccine series; if the infant received the hepatitis B vaccine on a normal schedule, then serologic testing would occur at about 9 to 12 months of age. Deferring the anti-HBs testing until after 9 months of age is important, since these infants may have residual anti-HBs out to 9 months from the hepatitis B immune globulin received at birth.[13,15,56] Testing of anti-HBc in infants should be avoided, since maternal anti-HBc may persist for at least 24 months.[13] For all ages, following any dose of hepatitis B vaccine, if HBsAg testing is needed to evaluate for active infection, the HBsAg test should be deferred for at least 1 month after receipt of a hepatitis B vaccine dose since the recombinant HBsAg in the hepatitis B vaccines can cause a transient false-positive HBsAg test for up to 18 days after vaccination.[56,57,58,59]
Interpretation of Postvaccination Serologic Testing
Anti-HBs levels of 10 mIU/mL or greater have been shown to strongly correlate with protection against HBV infection, although that exact threshold may vary from assay to assay.[60,61] As such, those with anti-HBs levels of at least 10 mIU/mL following hepatitis B immunization are considered immune to HBV and protected against infection with HBV.[13,14,15,61] For assays that utilize a cutoff different than 10 mIU/mL, it is important to refer to the package insert of the test used to appropriately interpret the results and determine the correct level of anti-HBs antibodies.[60,61]
Repeat Postvaccination Serologic Testing
Given the higher incidence of HBV infection among patients on long-term dialysis, patients undergoing outpatient hemodialysis should have anti-HBs testing yearly.[15,62] If anti-HBs levels fall below 10 mIU/mL, a booster dose of hepatitis B vaccine should be administered. In this setting, serologic testing to assess response is not recommended at 1–2 months.[15] The need for repeat postvaccination serologic testing has not been established in other populations at high risk for HBV acquisition, such as persons with HIV, hematopoietic stem-cell transplant recipients, and those receiving chemotherapy or other immunosuppressive drugs.[15] In these populations, the ACIP recommends consideration of annual anti-HBs testing with booster dose vaccination for persons at ongoing risk for HBV acquisition.[15]
Testing Health Care Workers Vaccinated in the Past
The ACIP suggests that health care institutions consider assessing preexposure immunity to HBV in all health care workers at the time of hire, regardless of vaccination status.[15] For health care workers with prior documentation of hepatitis B vaccine, testing for anti-HBs levels should be performed. If anti-HBs levels are 10 mIU/mL or greater, the health care worker is considered immune, and no HBV postexposure prophylaxis is needed following a potential exposure.[15] Health care workers with previous immunization against HBV and anti-HBs levels less than 10 mIU/mL should receive a one-time dose of hepatitis B vaccine, followed by postvaccination serologic testing 1–2 months later.[15] If the anti-HBs level remains less than 10 mIU/mL, administration of the complete hepatitis B vaccine series is recommended, again followed by postvaccination serologic testing. If, after repeat hepatitis B vaccination, the health care worker fails to mount a protective immune response (defined as anti-HBs levels 10 mIU/mL or greater), they should be counseled on the need for postexposure prophylaxis following exposure.[15] If a health care institution decides against measuring anti-HBs levels in their health care workers, they should ensure the health care workers seek timely evaluation for postexposure prophylaxis and assessment after any potential occupational exposure to HBV.[15]
Management of HBV Vaccine Nonresponders
Approach to HBV Vaccine Nonresponders in the General Population
Approximately 5 to 10% of immunized individuals fail to develop a protective antibody response (HBsAb level less than 10 mIU/mL) after a complete initial hepatitis B vaccine series. For persons who fail to generate adequate antibody levels in response to a primary hepatitis B vaccine series, revaccination can achieve a protective response at least half of the time.[15,63,64,65] The following summarizes CDC-recommended options for revaccination of hepatitis B vaccine nonresponders (in the general population).
- Administer a single hepatitis B vaccine dose followed by anti-HBs testing 1-2 months later, with completion of the second full series if repeat anti-HBs remains less than 10 mIU/mL, or
- Repeat vaccination with a second full 3-dose hepatitis B vaccine series, or
- Repeat vaccination with a 2-dose series of Heplisav-B.
Nonresponders to a second vaccine series are unlikely to develop a protective response to further doses of vaccine.[66]
Approach to HBV Vaccine Nonresponders in Key Populations
The following are recommendations for the approach to persons who do not respond to the initial hepatitis B vaccine series. Most of these recommendations are based on guidance from the CDC and ACIP, and focus on groups for which postvaccination serologic testing is recommended.[15]
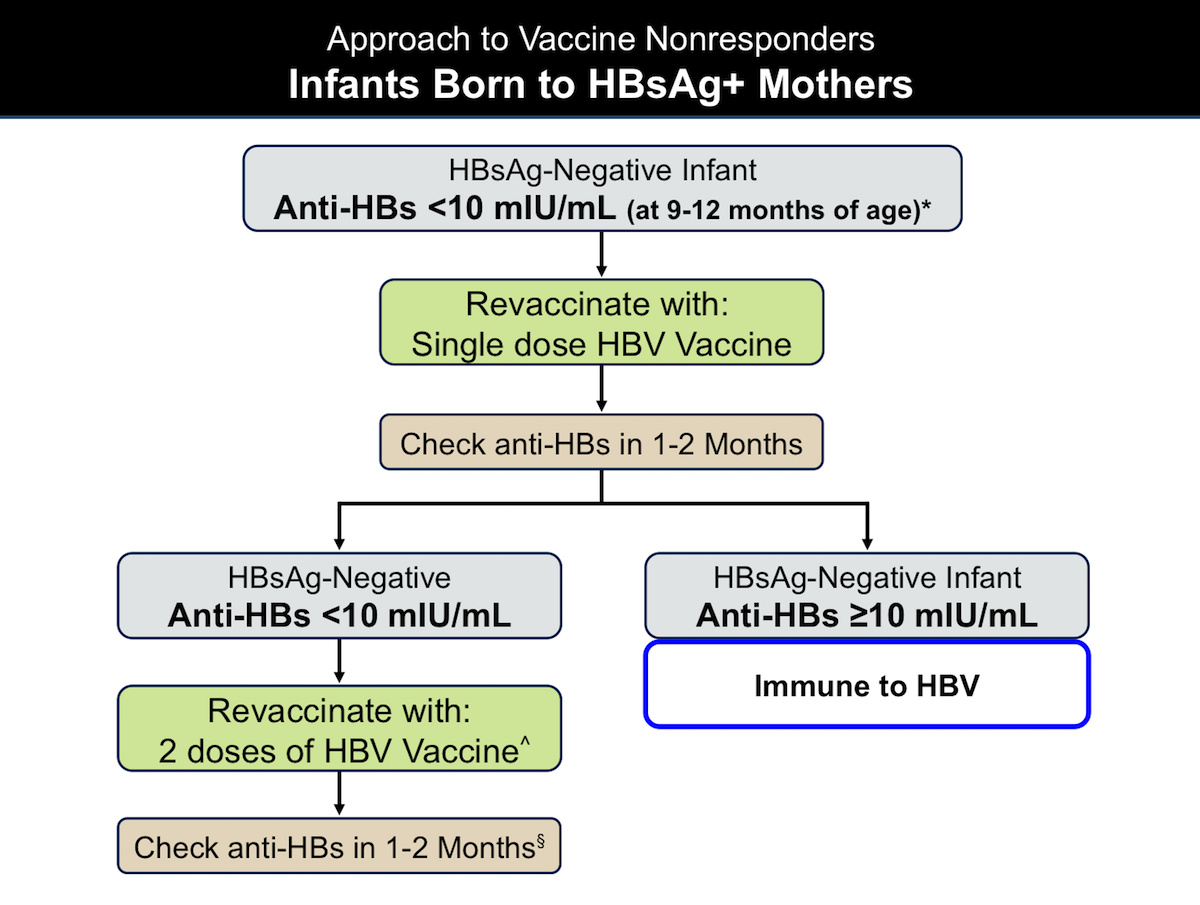
- Infants Born to HBsAg-Positive Mothers: In most circumstances, the approach to HBsAg-negative infants who were born to an HBsAg-positive mother requires a stepwise approach (Figure 10).[15] If infant serologic testing at 9–12 months of age shows the infant did not respond to the initial hepatitis B vaccine series (anti-HBs level less than 10 mIU/mL), they should receive 1 additional dose of hepatitis B vaccine, followed by repeat serologic testing 1–2 months later.[15] If, at that point, the infant’s anti-HBs level remains less than 10 mIU/mL, they should receive two additional doses of hepatitis B vaccine to complete a second 3-dose series.[15] Serologic testing (anti-HBs) should be performed 1–2 months after completion of the second hepatitis B vaccine series.[15] Alternatively, based on family preference and clinical circumstances, it is reasonable to give a full repeat 3-dose vaccine series to infants who did not respond to the initial vaccine series, with repeat serologic testing 1–2 months after the final dose of the vaccine series.[15]
- Health Care Workers: All health care workers who receive hepatitis B vaccination should have postvaccination serologic testing; vaccine nonresponders need further management (Figure 11).[15] Previously vaccinated health care personnel with an anti-HBs level of less than 10 mIU/mL should receive one additional dose of hepatitis B vaccine, followed by repeat serologic testing in 1 to 2 months.[15] If the anti-HBs titer remains less than 10 mIU/mL following a booster dose, two additional doses of vaccine should be administered, followed by repeat anti-HBs serologic screening 1–2 months after the final dose of vaccine.[15] As with infants, health care workers with anti-HBs less than 10 mIU/mL may find it more practical to receive a second complete hepatitis B vaccine series followed by repeat serologic testing at 1–2 months, as opposed to the stepwise strategy outlined above that begins with giving one dose.[15] In addition, the two-dose series of Heplisav-B should be considered in health care workers who require revaccination.[15] In a study of health care workers who did not respond to at least 5 doses of hepatitis B vaccine (Engerix-B or Recombivax), 91% (43 of 47) developed seroprotective responses after 2 doses of Heplisav-B.[67]
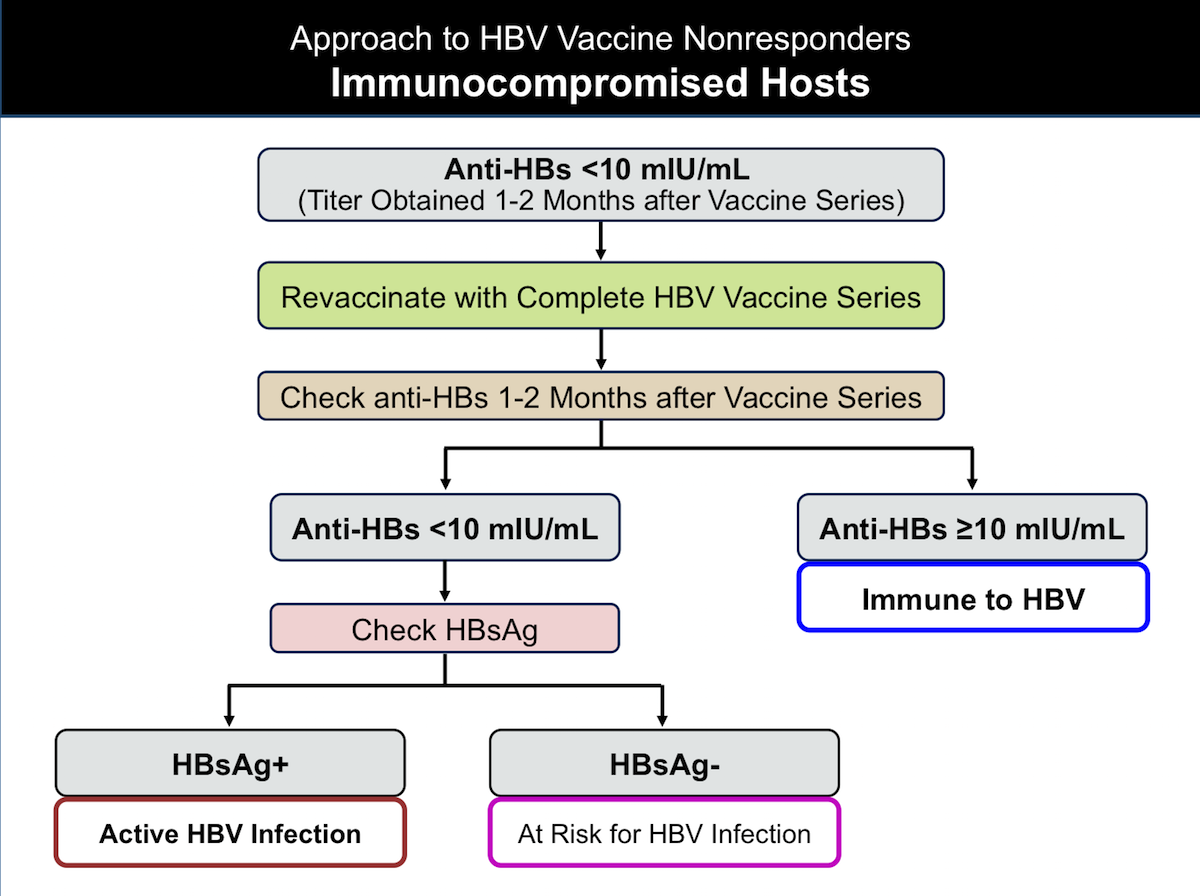
- Immunocompromised Adults: Hematopoietic stem-cell transplant recipients, persons with HIV, and persons receiving immunosuppressant medications who are HBsAg-negative and do not respond to initial hepatitis B vaccination (anti-HBs less than 10 mIU/mL 1–2 months after completing the initial series) should receive a second complete hepatitis B vaccine series, making certain all doses are given on schedule (Figure 12).[15] For persons with HIV who failed prior Engerix-B or Recombivax-HB, guidelines recommend revaccination using the two-dose Heplisav-B vaccine series, with consideration for a third dose of Heplisav-B at 24 weeks.[30,33] For all immunocompromised persons, anti-HBs testing should be performed again, ideally 1–2 months after completing the second vaccine series.[15] If the anti-HBs concentration remains less than 10 mIU/mL, then HBsAg testing should be performed to determine whether active HBV infection is the cause of vaccine nonresponse.[15] If the HBsAg test is negative, the person should be considered at risk of acquiring HBV infection, and they should receive counseling regarding the prevention of HBV infection.[15] Persons who test positive for HBsAg should be considered to have HBV infection and should receive further evaluation, management, and counseling.[15] Administering more than two complete hepatitis B vaccine series is generally not recommended for this population.
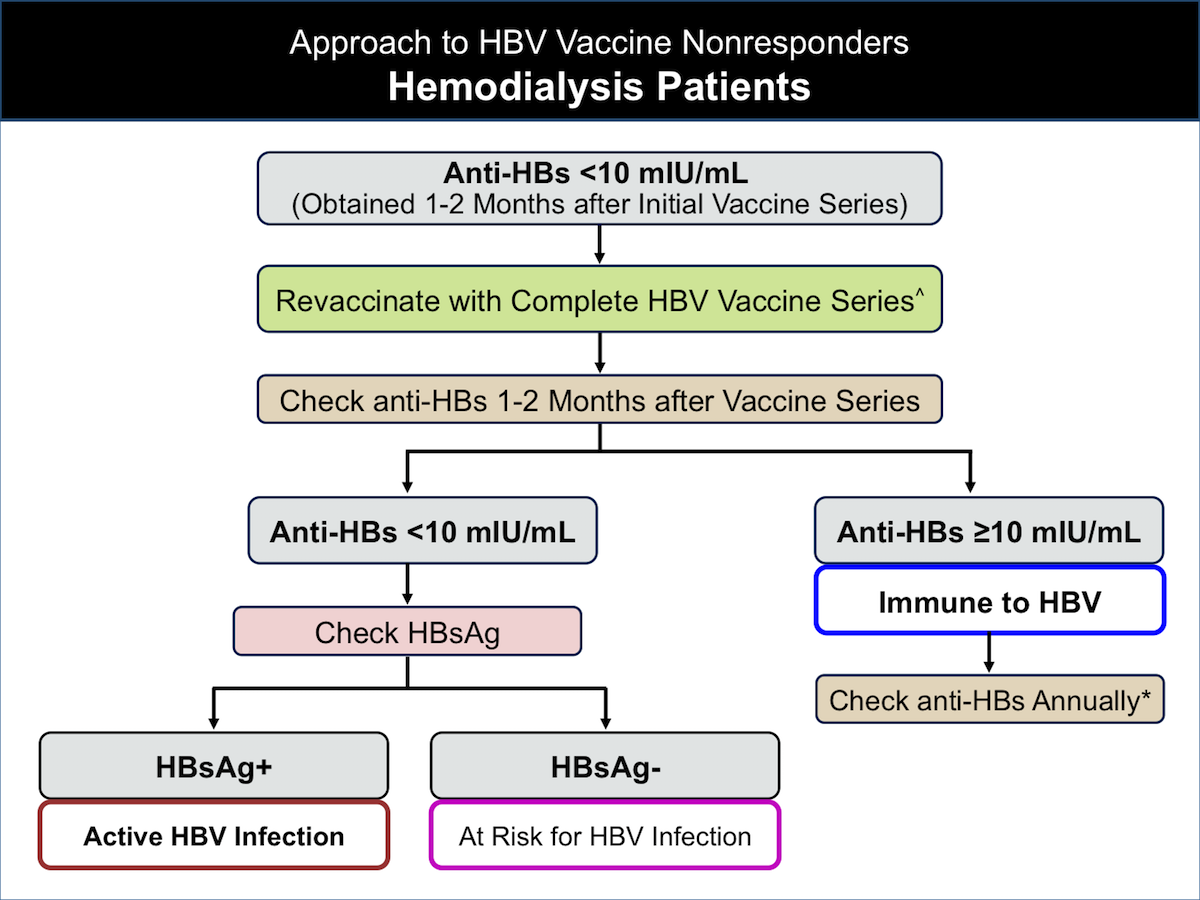
- Hemodialysis Patients: Hemodialysis patients who do not respond to the hepatitis B vaccine should be managed similar to other immunocompromised adults, with the exception that hemodialysis patients who respond to the second vaccine series should undergo yearly anti-HBs screening (Figure 13).[14,27] If anti-HBs levels fall below 10 mIU/mL, a booster dose of hepatitis B vaccine should be administered.[15] In this setting, given the frequency of anti-HBs screening, serologic testing to assess response to additional doses of vaccine is not recommended at 1-2 months after the booster dose.[14,15] For all persons who do not respond to a second hepatitis B vaccine series, additional testing with HBsAg and anti-HBc should be considered to evaluate for active HBV infection. In the setting of an isolated anti-HBc, testing for HBV DNA should be considered to rule out occult HBV.
Strategies for the Management of HBV Vaccine Nonresponders
Several additional strategies have been utilized in managing persons who do not respond to the initial hepatitis B vaccine series, but none of these have been established to have better efficacy in the general population than the strategy outlined in the CDC recommendations for hepatitis B vaccine nonresponders.[68] The following summarizes strategies that have been employed in the management of hepatitis B vaccine nonresponders.
- Increased Vaccine Doses or Antigen per Dose: There are several studies that have evaluated the efficacy of using increased hepatitis B vaccine doses for the management of nonresponders. One study of 48 healthy adult nonresponders showed that revaccination with a double dose of combined hepatitis A and B vaccine (Twinrix) led to protective titers (anti-HBs levels 10 mIU/mL or greater) in 95% of study subjects.[69] A similar study evaluated the use of double-dose versus single-dose hepatitis B vaccine in health care workers who did not previously respond to hepatitis B vaccination. In this study, 97.8% of those receiving the double-dose and 89.6% of those receiving the single dose developed anti-HBs titers of 10 mIU/mL or greater; this difference, however, was not statistically significant.[70] Moreover, a systematic review and meta-analysis of vaccine options for adults who did not respond to prior hepatitis B vaccination showed no statistical difference in rates of protective anti-HBs levels between those who were revaccinated with standard-dose hepatitis B vaccine versus those who received a double dose of hepatitis B vaccine.[68]
- Intradermal Administration: There are limited data supporting the enhanced immunogenicity of intradermal versus intramuscular hepatitis B vaccination. In one study of 50 previously vaccinated hemodialysis patients without protective anti-HBs levels, revaccination with intradermal hepatitis B vaccine, in comparison to intramuscular hepatitis B vaccine, yielded statistically higher rates of seroprotection at 1, 12, and 20 months.[71] A similar study of hepatitis B vaccine nonresponders on hemodialysis showed significantly higher seroconversion rates (79% vs 40%) among hemodialysis patients who received weekly intradermal vaccine for 8 weeks versus those who received intramuscular vaccine at 1 and 8 weeks.[72] In a study involving 42 patients with chronic liver disease who failed initial intramuscular hepatitis B vaccination, 69% had an immunologic response (anti-HBs10 mIU/mL or greater) after repeat vaccination with up to three doses of intradermal vaccine.[73] In clinical practice, however, intradermal hepatis B vaccines are not routinely used, primarily because of lack of FDA approval for this use and the limited availability of skilled personnel to administer intradermal vaccines.
Summary Points
- In the United States, overall hepatitis B vaccine delivery and coverage rates among adults are low, despite high rates of vaccine acceptance among adults who are offered the vaccine.
- All infants, children, adolescents younger than 19 years of age, adults 19 to 59 years of age, and adults 60 years of age and older with risk factors for HBV should receive hepatitis B vaccination. Adults 60 years of age and older without risk factors for HBV may receive the hepatitis B vaccine.
- In general, prevaccination serologic testing is not indicated unless the person is at high risk for HBV infection.
- There are three single-antigen hepatitis B vaccines and one hepatitis A-hepatitis B combination vaccine approved for adults in the United States. The ACIP does not provide preferential guidance on which vaccine to use, although many experts prefer Heplisav-B owing to high rates of seroprotection and a convenient 2-dose schedule. All can be used in pregnant women.
- In infants, only single-antigen HBV vaccines (Engerix-B or Recombivax-HB) should be used for the birth-dose hepatitis B vaccine, but combination vaccines can be used to complete the hepatitis B vaccine series.
- Overall response to hepatitis B vaccination is good, with greater than 90% of healthy adults achieving protective immunity after three doses of vaccine, defined as an HBsAb level of 10 mIU/mL or greater.
- Age greater than 40 years, male sex, obesity, diabetes, tobacco smoking, chronic hepatitis C infection, alcohol use disorder, renal disease, HIV infection, celiac disease, other immune-compromising conditions, and certain genetic determinants have been associated with suboptimal response to hepatitis B vaccination.
- Postvaccination serologic testing is indicated for the following groups: infants born to HBsAg-positive mothers or mothers of unknown HBsAg status, health care workers and public safety workers at risk for exposure to blood or body fluids, persons on hemodialysis, persons with HIV, other immunocompromised persons, and sex partners of HBsAg-positive persons.
- For the estimated 5 to 10% of individuals who fail to develop a protective antibody response to an initial 3-dose hepatitis B vaccine series, a fourth vaccine dose or a second full 3-dose revaccination series can achieve a protective response in at least 50% of these persons.
- Novel adjuvants, double-dose vaccinations, intradermal vaccines, and vaccines containing proteins in the pre-S1 and pre-S2 regions on the HBV envelope have been used to elicit better immune responses in vaccine nonresponders.
Citations
- 1.Global hepatitis report 2024: action for access in low- and middle-income countries. Geneva: World Health Organization; 2024:1-239.[WHO] -
- 2.Weng MK, Doshani M, Khan MA, et al. Universal Hepatitis B Vaccination in Adults Aged 19-59 Years: Updated Recommendations of the Advisory Committee on Immunization Practices - United States, 2022. MMWR Morb Mortal Wkly Rep. 2022;71:477-83.[PubMed Abstract] -
- 3.Zanetti AR, Van Damme P, Shouval D. The global impact of vaccination against hepatitis B: a historical overview. Vaccine. 2008;26:6266-73.[PubMed Abstract] -
- 4.Stephenne J. Development and production aspects of a recombinant yeast-derived hepatitis B vaccine. Vaccine. 1990;8 Suppl:S69-73; discussion S79-80.[PubMed Abstract] -
- 5.Szmuness W, Stevens CE, Harley EJ, et al. Hepatitis B vaccine: demonstration of efficacy in a controlled clinical trial in a high-risk population in the United States. N Engl J Med. 1980;303:833-41.[PubMed Abstract] -
- 6.Young MD, Schneider DL, Zuckerman AJ, Du W, Dickson B, Maddrey WC. Adult hepatitis B vaccination using a novel triple antigen recombinant vaccine. Hepatology. 2001;34:372-6.[PubMed Abstract] -
- 7.Schillie S, Harris A, Link-Gelles R, Romero J, Ward J, Nelson N. Recommendations of the Advisory Committee on Immunization Practices for Use of a Hepatitis B Vaccine with a Novel Adjuvant. MMWR Morb Mortal Wkly Rep. 2018;67:455-8.[PubMed Abstract] -
- 8.Lu PJ, Hung MC, Srivastav A, et al. Surveillance of Vaccination Coverage Among Adult Populations -United States, 2018. MMWR Surveill Summ. 2021;70:1-26.[PubMed Abstract] -
- 9.Weinbaum CM, Lyerla R, Mackellar DA, et al. The Young Men's Survey phase II: hepatitis B immunization and infection among young men who have sex with men. Am J Public Health. 2008;98:839-45.[PubMed Abstract] -
- 10.Hill HA, Yankey D, Elam-Evans LD, et al. Decline in Vaccination Coverage by Age 24 Months and Vaccination Inequities Among Children Born in 2020 and 2021 - National Immunization Survey-Child, United States, 2021-2023. MMWR Morb Mortal Wkly Rep. 2024;73:844-53.[PubMed Abstract] -
- 11.Pingali C, Yankey D, Chen M, et al. National Vaccination Coverage Among Adolescents Aged 13-17 Years - National Immunization Survey-Teen, United States, 2023. MMWR Morb Mortal Wkly Rep. 2024;73:708-14.[PubMed Abstract] -
- 12.Centers for Disease Control and Prevention (CDC).. Use of hepatitis B vaccination for adults with diabetes mellitus: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2011;60:1709-11.[PubMed Abstract] -
- 13.Mast EE, Margolis HS, Fiore AE, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP) part 1: immunization of infants, children, and adolescents. MMWR Recomm Rep. 2005;54:1-31.[PubMed Abstract] -
- 14.Mast EE, Weinbaum CM, Fiore AE, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP) Part II: immunization of adults. MMWR Recomm Rep. 2006;55:1-33.[PubMed Abstract] -
- 15.Schillie S, Vellozzi C, Reingold A, et al. Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2018;67:1-31.[PubMed Abstract] -
- 16.Centers for Disease Control (CDC). Recommendation of the Immunization Practices Advisory Committee (ACIP). Inactivated hepatitis B virus vaccine. MMWR Morb Mortal Wkly Rep. 1982;31:317-22, 327-8.[PubMed Abstract] -
- 17.Iqbal K, Klevens RM, Kainer MA, et al. Epidemiology of Acute Hepatitis B in the United States From Population-Based Surveillance, 2006-2011. Clin Infect Dis. 2015;61:584-92.[PubMed Abstract] -
- 18.Bradley H, Hall E, Asher A, et al. Estimated number of people who inject drugs in the United States. Clin Infect Dis. 2022 Jul 6. Online ahead of print.[PubMed Abstract] -
- 19.Centers for Disease Control and Prevention (CDC). 2023 Viral Hepatitis Surveillance Report—Hepatitis B. Published April 15, 2025.[CDC] -
- 20.Blostein J, Clark PA. Cost-effectiveness of preimmunization hepatitis B screening in high-risk adolescents. Public Health Rep. 2001;116:165-8.[PubMed Abstract] -
- 21.Centers for Disease Control and Prevention. Hepatitis B vaccination of inmates in correctional facilities--Texas, 2000-2002. MMWR Morb Mortal Wkly Rep. 2004;53:681-3.[PubMed Abstract] -
- 22.Hu Y, Grau LE, Scott G, et al. Economic evaluation of delivering hepatitis B vaccine to injection drug users. Am J Prev Med. 2008;35:25-32.[PubMed Abstract] -
- 23.Weinbaum CM, Williams I, Mast EE, et al. Recommendations for identification and public health management of persons with chronic hepatitis B virus infection. MMWR Recomm Rep. 2008;57:1-20.[PubMed Abstract] -
- 24.Liang JL, Tiwari T, Moro P, et al. Prevention of Pertussis, Tetanus, and Diphtheria with Vaccines in the United States: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2018;67:1-44.[PubMed Abstract] -
- 25.Sandul AL, Rapposelli K, Nyendak M, Kim M. Updated Recommendation for Universal Hepatitis B Vaccination in Adults Aged 19-59 Years - United States, 2024. MMWR Morb Mortal Wkly Rep. 2024;73:1106.[PubMed Abstract] -
- 26.Janssen RS, Mangoo-Karim R, Pergola PE, et al. Immunogenicity and safety of an investigational hepatitis B vaccine with a toll-like receptor 9 agonist adjuvant (HBsAg-1018) compared with a licensed hepatitis B vaccine in patients with chronic kidney disease. Vaccine. 2013;31:5306-13.[PubMed Abstract] -
- 27.Centers for Disease Control and Prevention. Guidelines for Vaccinating Kidney Dialysis Patients and Patients with Chronic Kidney Disease. December 2012.[CDC] -
- 28.Tung J, Carlisle E, Smieja M, Kim PT, Lee CH. A randomized clinical trial of immunization with combined hepatitis A and B versus hepatitis B alone for hepatitis B seroprotection in hemodialysis patients. Am J Kidney Dis. 2010;56:713-9.[PubMed Abstract] -
- 29.Awad AM, Ntoso A, Connaire JJ, et al. An open-label, single-arm study evaluating the immunogenicity and safety of the hepatitis B vaccine HepB-CpG (HEPLISAV-B®) in adults receiving hemodialysis. Vaccine. 2021;39:3346-52.[PubMed Abstract] -
- 30.Panel on Opportunistic Infections in Adults and Adolescents with HIV. Guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV: recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. Hepatitis B virus infection. Last Updated: December 16, 2024.[HIV.gov] -
- 31.Marks KM, Kang M, Umbleja T, et al. Immunogenicity and Safety of Hepatitis B Virus (HBV) Vaccine With a Toll-Like Receptor 9 Agonist Adjuvant in HBV Vaccine-Naïve People With Human Immunodeficiency Virus. Clin Infect Dis. 2023;77:414-8.[PubMed Abstract] -
- 32.Lee JH, Hong S, Im JH, Lee JS, Baek JH, Kwon HY. Systematic review and meta-analysis of immune response of double dose of hepatitis B vaccination in HIV-infected patients. Vaccine. 2020;38:3995-4000.[PubMed Abstract] -
- 33.Marks KM, Kang M, Umbleja T, et al. HepB-CpG vs HepB-Alum Vaccine in People With HIV and Prior Vaccine Nonresponse: The BEe-HIVe Randomized Clinical Trial. JAMA. 2024 Dec 1. Online ahead of print.[PubMed Abstract] -
- 34.Zajac BA, West DJ, McAleer WJ, Scolnick EM. Overview of clinical studies with hepatitis B vaccine made by recombinant DNA. J Infect. 1986;13 Suppl A:39-45.[PubMed Abstract] -
- 35.Averhoff F, Mahoney F, Coleman P, Schatz G, Hurwitz E, Margolis H. Immunogenicity of hepatitis B Vaccines. Implications for persons at occupational risk of hepatitis B virus infection. Am J Prev Med. 1998;15:1-8.[PubMed Abstract] -
- 36.André FE. Summary of safety and efficacy data on a yeast-derived hepatitis B vaccine. Am J Med. 1989;87:14S-20S.[PubMed Abstract] -
- 37.Joines RW, Blatter M, Abraham B, et al. A prospective, randomized, comparative US trial of a combination hepatitis A and B vaccine (Twinrix) with corresponding monovalent vaccines (Havrix and Engerix-B) in adults. Vaccine. 2001;19:4710-9.[PubMed Abstract] -
- 38.Jackson S, Lentino J, Kopp J, et al. Immunogenicity of a two-dose investigational hepatitis B vaccine, HBsAg-1018, using a toll-like receptor 9 agonist adjuvant compared with a licensed hepatitis B vaccine in adults. Vaccine. 2018;36:668-674.[PubMed Abstract] -
- 39.Heyward WL, Kyle M, Blumenau J, et al. Immunogenicity and safety of an investigational hepatitis B vaccine with a Toll-like receptor 9 agonist adjuvant (HBsAg-1018) compared to a licensed hepatitis B vaccine in healthy adults 40-70 years of age. Vaccine. 2013;31:5300-5.[PubMed Abstract] -
- 40.Halperin SA, Ward B, Cooper C, et al. Comparison of safety and immunogenicity of two doses of investigational hepatitis B virus surface antigen co-administered with an immunostimulatory phosphorothioate oligodeoxyribonucleotide and three doses of a licensed hepatitis B vaccine in healthy adults 18-55 years of age. Vaccine. 2012;30:2556-63.[PubMed Abstract] -
- 41.Halperin SA, Dobson S, McNeil S, et al. Comparison of the safety and immunogenicity of hepatitis B virus surface antigen co-administered with an immunostimulatory phosphorothioate oligonucleotide and a licensed hepatitis B vaccine in healthy young adults. Vaccine. 2006;24:20-6.[PubMed Abstract] -
- 42.Sablan BP, Kim DJ, Barzaga NG, et al. Demonstration of safety and enhanced seroprotection against hepatitis B with investigational HBsAg-1018 ISS vaccine compared to a licensed hepatitis B vaccine. Vaccine. 2012;30:2689-96.[PubMed Abstract] -
- 43.Bruguera M, Cremades M, Salinas R, Costa J, Grau M, Sans J. Impaired response to recombinant hepatitis B vaccine in HIV-infected persons. J Clin Gastroenterol. 1992;14:27-30.[PubMed Abstract] -
- 44.Lacson E, Teng M, Ong J, Vienneau L, Ofsthun N, Lazarus JM. Antibody response to Engerix-B and Recombivax-HB hepatitis B vaccination in end-stage renal disease. Hemodial Int. 2005;9:367-75.[PubMed Abstract] -
- 45.Shaw FE Jr, Guess HA, Roets JM, et al. Effect of anatomic injection site, age and smoking on the immune response to hepatitis B vaccination. Vaccine. 1989;7:425-30.[PubMed Abstract] -
- 46.Mendenhall C, Roselle GA, Lybecker LA, et al. Hepatitis B vaccination. Response of alcoholic with and without liver injury. Dig Dis Sci. 1988;33:263-9.[PubMed Abstract] -
- 47.Alper CA, Kruskall MS, Marcus-Bagley D, et al. Genetic prediction of nonresponse to hepatitis B vaccine. N Engl J Med. 1989;321:708-12.[PubMed Abstract] -
- 48.Langö-Warensjö A, Cardell K, Lindblom B. Haplotypes comprising subtypes of the DQB1*06 allele direct the antibody response after immunisation with hepatitis B surface antigen. Tissue Antigens. 1998;52:374-80.[PubMed Abstract] -
- 49.Zanetti AR, Mariano A, Romanò L, et al. Long-term immunogenicity of hepatitis B vaccination and policy for booster: an Italian multicentre study. Lancet. 2005;366:1379-84.[PubMed Abstract] -
- 50.Fitzsimons D, François G, Hall A, et al. Long-term efficacy of hepatitis B vaccine, booster policy, and impact of hepatitis B virus mutants. Vaccine. 2005;23:4158-66.[PubMed Abstract] -
- 51.Bauer T, Jilg W. Hepatitis B surface antigen-specific T and B cell memory in individuals who had lost protective antibodies after hepatitis B vaccination. Vaccine. 2006;24:572-7.[PubMed Abstract] -
- 52.Gara N, Abdalla A, Rivera E, et al. Durability of antibody response against hepatitis B virus in healthcare workers vaccinated as adults. Clin Infect Dis. 2015;60:505-13.[PubMed Abstract] -
- 53.Bruce MG, Bruden D, Hurlburt D, et al. Protection and antibody levels 35 years after primary series with hepatitis B vaccine and response to a booster dose. Hepatology. 2022 Mar 23. Online ahead of print.[PubMed Abstract] -
- 54.Middleman AB, Baker CJ, Kozinetz CA, et al. Duration of protection after infant hepatitis B vaccination series. Pediatrics. 2014;133:e1500-7.[PubMed Abstract] -
- 55.Bruce MG, Bruden D, Hurlburt D, et al. Antibody Levels and Protection After Hepatitis B Vaccine: Results of a 30-Year Follow-up Study and Response to a Booster Dose. J Infect Dis. 2016;214:16-22.[PubMed Abstract] -
- 56.Schillie S, Murphy TV, Fenlon N, Ko S, Ward JW. Update: Shortened Interval for Postvaccination Serologic Testing of Infants Born to Hepatitis B-Infected Mothers. MMWR Morb Mortal Wkly Rep. 2015;64:1118-20.[PubMed Abstract] -
- 57.Challapalli M, Naidu V, Cunningham DG. Hepatitis B surface antigenemia in a newborn infant after vaccination. Pediatr Infect Dis J. 1993;12:408-9.[PubMed Abstract] -
- 58.Fleischer L, Syed SS. Hepatitis B surface antigenemia in a neonate following vaccination with Pediarix. Clin Pediatr (Phila). 2009;48:311-2.[PubMed Abstract] -
- 59.Onuigbo MA, Nesbit A, Weisenbeck J, Hurlburt J. Hepatitis B surface antigenemia following recombinant Engerix B hepatitis B vaccine in an 81-year-old ESRD patient on hemodialysis. Ren Fail. 2010;32:531-2.[PubMed Abstract] -
- 60.Hadler SC, Francis DP, Maynard JE, et al. Long-term immunogenicity and efficacy of hepatitis B vaccine in homosexual men. N Engl J Med. 1986;315:209-14.[PubMed Abstract] -
- 61.Jack AD, Hall AJ, Maine N, Mendy M, Whittle HC. What level of hepatitis B antibody is protective? J Infect Dis. 1999;179:489-92.[PubMed Abstract] -
- 62.Finelli L, Miller JT, Tokars JI, Alter MJ, Arduino MJ. National surveillance of dialysis-associated diseases in the United States, 2002. Semin Dial. 2005;18:52-61.[PubMed Abstract] -
- 63.Goldwater PN. Randomized, comparative trial of 20 micrograms vs 40 micrograms Engerix B vaccine in hepatitis B vaccine non-responders. Vaccine. 1997;15:353-6.[PubMed Abstract] -
- 64.Bertino JS Jr, Tirrell P, Greenberg RN, et al. A comparative trial of standard or high-dose S subunit recombinant hepatitis B vaccine versus a vaccine containing S subunit, pre-S1, and pre-S2 particles for revaccination of healthy adult nonresponders. J Infect Dis. 1997;175:678-81.[PubMed Abstract] -
- 65.Halperin SA, Ward BJ, Dionne M, et al. Immunogenicity of an investigational hepatitis B vaccine (hepatitis B surface antigen co-administered with an immunostimulatory phosphorothioate oligodeoxyribonucleotide) in nonresponders to licensed hepatitis B vaccine. Hum Vaccin Immunother. 2013;9:1438-44.[PubMed Abstract] -
- 66.Yu AS, Cheung RC, Keeffe EB. Hepatitis B vaccines. Clin Liver Dis. 2004;8:283-300.[PubMed Abstract] -
- 67.Russ RK, Vandehei HM, Golovkina MI, Mogallapalli H, Caldera F, Hayney MS. Hepatitis B-CpG Vaccine Series for Healthcare Workers Who Are Hepatitis B Vaccine Nonresponders. Clin Infect Dis. 2024;79:562-3.[PubMed Abstract] -
- 68.David MC, Ha SH, Paynter S, Lau C. A systematic review and meta-analysis of management options for adults who respond poorly to hepatitis B vaccination. Vaccine. 2015;33:6564-9.[PubMed Abstract] -
- 69.Cardell K, Akerlind B, Sällberg M, Frydén A. Excellent response rate to a double dose of the combined hepatitis A and B vaccine in previous nonresponders to hepatitis B vaccine. J Infect Dis. 2008;198:299-304.[PubMed Abstract] -
- 70.Joukar F, Mansour-Ghanaei F, Naghipour MR, Asgharnezhad M. Immune Responses to Single-Dose Versus Double-Dose Hepatitis B Vaccines in Healthcare Workers not Responding to the Primary Vaccine Series: A Randomized Clinical Trial. Hepat Mon. 2016;16:e32799.[PubMed Abstract] -
- 71.Fabrizi F, Andrulli S, Bacchini G, Corti M, Locatelli F. Intradermal versus intramuscular hepatitis b re-vaccination in non-responsive chronic dialysis patients: a prospective randomized study with cost-effectiveness evaluation. Nephrol Dial Transplant. 1997;12:1204-11.[PubMed Abstract] -
- 72.Barraclough KA, Wiggins KJ, Hawley CM, et al. Intradermal versus intramuscular hepatitis B vaccination in hemodialysis patients: a prospective open-label randomized controlled trial in nonresponders to primary vaccination. Am J Kidney Dis. 2009;54:95-103.[PubMed Abstract] -
- 73.Dhillon S, Moore C, Li SD, et al. Efficacy of high-dose intra-dermal hepatitis B virus vaccine in previous vaccination non-responders with chronic liver disease. Dig Dis Sci. 2012;57:215-20.[PubMed Abstract] -
Additional References
- A Two-Dose Hepatitis B Vaccine for Adults (Heplisav-B). JAMA. 2018;319:822-3.[PubMed Abstract] -
- Barry M, Cooper C. Review of hepatitis B surface antigen-1018 ISS adjuvant-containing vaccine safety and efficacy. Expert Opin Biol Ther. 2007;7:1731-7.[PubMed Abstract] -
- Bruce MG, Bruden D, Hurlburt D, et al. Protection and antibody levels 35 years after primary series with hepatitis B vaccine and response to a booster dose. Hepatology. 2022;76:1180-9.[PubMed Abstract] -
- Clemens R, Sänger R, Kruppenbacher J, et al. Booster immunization of low- and non-responders after a standard three dose hepatitis B vaccine schedule--results of a post-marketing surveillance. Vaccine. 1997;15:349-52.[PubMed Abstract] -
- Conners EE, Panagiotakopoulos L, Hofmeister MG, et al. Screening and Testing for Hepatitis B Virus Infection: CDC Recommendations - United States, 2023. MMWR Recomm Rep. 2023;72:1-25.[PubMed Abstract] -
- Fonseca MO, Pang LW, de Paula Cavalheiro N, Barone AA, Heloisa Lopes M. Randomized trial of recombinant hepatitis B vaccine in HIV-infected adult patients comparing a standard dose to a double dose. Vaccine. 2005;23:2902-8.[PubMed Abstract] -
- Hill HA, Elam-Evans LD, Yankey D, Singleton JA, Kang Y. Vaccination Coverage Among Children Aged 19-35 Months - United States, 2017. MMWR Morb Mortal Wkly Rep. 2018;67:1123-8.[PubMed Abstract] -
- Hyer R, McGuire DK, Xing B, Jackson S, Janssen R. Safety of a two-dose investigational hepatitis B vaccine, HBsAg-1018, using a toll-like receptor 9 agonist adjuvant in adults. Vaccine. 2018;36:2604-2611.[PubMed Abstract] -
- Janssen JM, Heyward WL, Martin JT, Janssen RS. Immunogenicity and safety of an investigational hepatitis B vaccine with a Toll-like receptor 9 agonist adjuvant (HBsAg-1018) compared with a licensed hepatitis B vaccine in patients with chronic kidney disease and type 2 diabetes mellitus. Vaccine. 2015;33:833-7.[PubMed Abstract] -
- Kim HN, Harrington RD, Crane HM, Dhanireddy S, Dellit TH, Spach DH. Hepatitis B vaccination in HIV-infected adults: current evidence, recommendations and practical considerations. Int J STD AIDS. 2009;20:595-600.[PubMed Abstract] -
- Ko SC, Schillie SF, Walker T, et al. Hepatitis B vaccine response among infants born to hepatitis B surface antigen-positive women. Vaccine. 2014;32:2127-33.[PubMed Abstract] -
- Launay O, van der Vliet D, Rosenberg AR, et al. Safety and immunogenicity of 4 intramuscular double doses and 4 intradermal low doses vs standard hepatitis B vaccine regimen in adults with HIV-1: a randomized controlled trial. JAMA. 2011;305:1432-40.[PubMed Abstract] -
- Lu PJ, O'Halloran A, Kennedy ED, et al. Awareness among adults of vaccine-preventable diseases and recommended vaccinations, United States, 2015. Vaccine. 2017;35:3104-3115.[PubMed Abstract] -
- Marks KM, Kang M, Umbleja T, et al. Immunogenicity and Safety of Hepatitis B Virus (HBV) Vaccine With a Toll-Like Receptor 9 Agonist Adjuvant in HBV Vaccine-Naïve People With Human Immunodeficiency Virus. Clin Infect Dis. 2023;77:414-8. Extra[PubMed Abstract] -
- Nelson NP, Easterbrook PJ, McMahon BJ. Epidemiology of Hepatitis B Virus Infection and Impact of Vaccination on Disease. Clin Liver Dis. 2016;20:607-28.[PubMed Abstract] -
- Noh KW, Poland GA, Murray JA. Hepatitis B vaccine nonresponse and celiac disease. Am J Gastroenterol. 2003;98:2289-92.[PubMed Abstract] -
- Park SD, Markowitz J, Pettei M, et al. Failure to respond to hepatitis B vaccine in children with celiac disease. J Pediatr Gastroenterol Nutr. 2007;44:431-5.[PubMed Abstract] -
- Poland GA, Jacobson RM. Clinical practice: prevention of hepatitis B with the hepatitis B vaccine. N Engl J Med. 2004;351:2832-8.[PubMed Abstract] -
- Propst T, Propst A, Lhotta K, Vogel W, König P. Reinforced intradermal hepatitis B vaccination in hemodialysis patients is superior in antibody response to intramuscular or subcutaneous vaccination. Am J Kidney Dis. 1998;32:1041-5.[PubMed Abstract] -
- Rey D, Krantz V, Partisani M, et al. Increasing the number of hepatitis B vaccine injections augments anti-HBs response rate in HIV-infected patients. Effects on HIV-1 viral load. Vaccine. 2000;18:1161-5.[PubMed Abstract] -
- Rey D, Piroth L, Wendling MJ, et al. Safety and immunogenicity of double-dose versus standard-dose hepatitis B revaccination in non-responding adults with HIV-1 (ANRS HB04 B-BOOST): a multicentre, open-label, randomised controlled trial. Lancet Infect Dis. 2015;15:1283-91.[PubMed Abstract] -
- Russ RK, Vandehei HM, Golovkina MI, Mogallapalli H, Caldera F, Hayney MS. Hepatitis B-CpG Vaccine Series for Healthcare Workers Who Are Hepatitis B Vaccine Nonresponders. Clin Infect Dis. 2024;79:562-63.Eztra[PubMed Abstract] -
- Saco TV, Strauss AT, Ledford DK. Hepatitis B vaccine nonresponders: Possible mechanisms and solutions. Ann Allergy Asthma Immunol. 2018;121:320-327.[PubMed Abstract] -
- Shafran SD, Mashinter LD, Lindemulder A, Taylor GD, Chiu I. Poor efficacy of intradermal administration of recombinant hepatitis B virus immunization in HIV-infected individuals who fail to respond to intramuscular administration of hepatitis B virus vaccine. HIV Med. 2007;8:295-9.[PubMed Abstract] -
- Splawn LM, Bailey CA, Medina JP, Cho JC. Heplisav-B vaccination for the prevention of hepatitis B virus infection in adults in the United States. Drugs Today (Barc). 2018;54:399-405.[PubMed Abstract] -
- van den Berg R, van Hoogstraten I, van Agtmael M. Non-responsiveness to hepatitis B vaccination in HIV seropositive patients; possible causes and solutions. AIDS Rev. 2009;11:157-64.[PubMed Abstract] -
- Van Den Ende C, Marano C, Van Ahee A, Bunge EM, De Moerlooze L. The immunogenicity and safety of GSK's recombinant hepatitis B vaccine in adults: a systematic review of 30 years of experience. Expert Rev Vaccines. 2017;16:811-32.[PubMed Abstract] -
- Vesikari T, Langley JM, Segall N, et al. Immunogenicity and safety of a tri-antigenic versus a mono-antigenic hepatitis B vaccine in adults (PROTECT): a randomised, double-blind, phase 3 trial. Lancet Infect Dis. 2021;21:1271-81.[PubMed Abstract] -
- Walayat S, Ahmed Z, Martin D, Puli S, Cashman M, Dhillon S. Recent advances in vaccination of non-responders to standard dose hepatitis B virus vaccine. World J Hepatol. 2015;7:2503-9.[PubMed Abstract] -
- Weber DJ, Rutala WA, Samsa GP, Santimaw JE, Lemon SM. Obesity as a predictor of poor antibody response to hepatitis B plasma vaccine. JAMA. 1985;254:3187-9.[PubMed Abstract] -
- Yousaf F, Gandham S, Galler M, Spinowitz B, Charytan C. Systematic review of the efficacy and safety of intradermal versus intramuscular hepatitis B vaccination in end-stage renal disease population unresponsive to primary vaccination series. Ren Fail. 2015;37:1080-8.[PubMed Abstract] -
- Zuckerman JN, Sabin C, Craig FM, Williams A, Zuckerman AJ. Immune response to a new hepatitis B vaccine in healthcare workers who had not responded to standard vaccine: randomised double blind dose-response study. BMJ. 1997;314:329-33.[PubMed Abstract] -
Figures





^The two additional doses should be given on a regular vaccine schedule to complete the second HBV vaccine series.
§If anti-HBs remains <10 mIU/mL after repeat vaccination, there is no evidence for the benefit of giving additional vaccine doses.
Some experts recommend an alternative strategy of giving a second complete series (instead of the one initial dose of hepatitis B vaccine), followed by anti-HBs testing 1–2 months after the final dose.
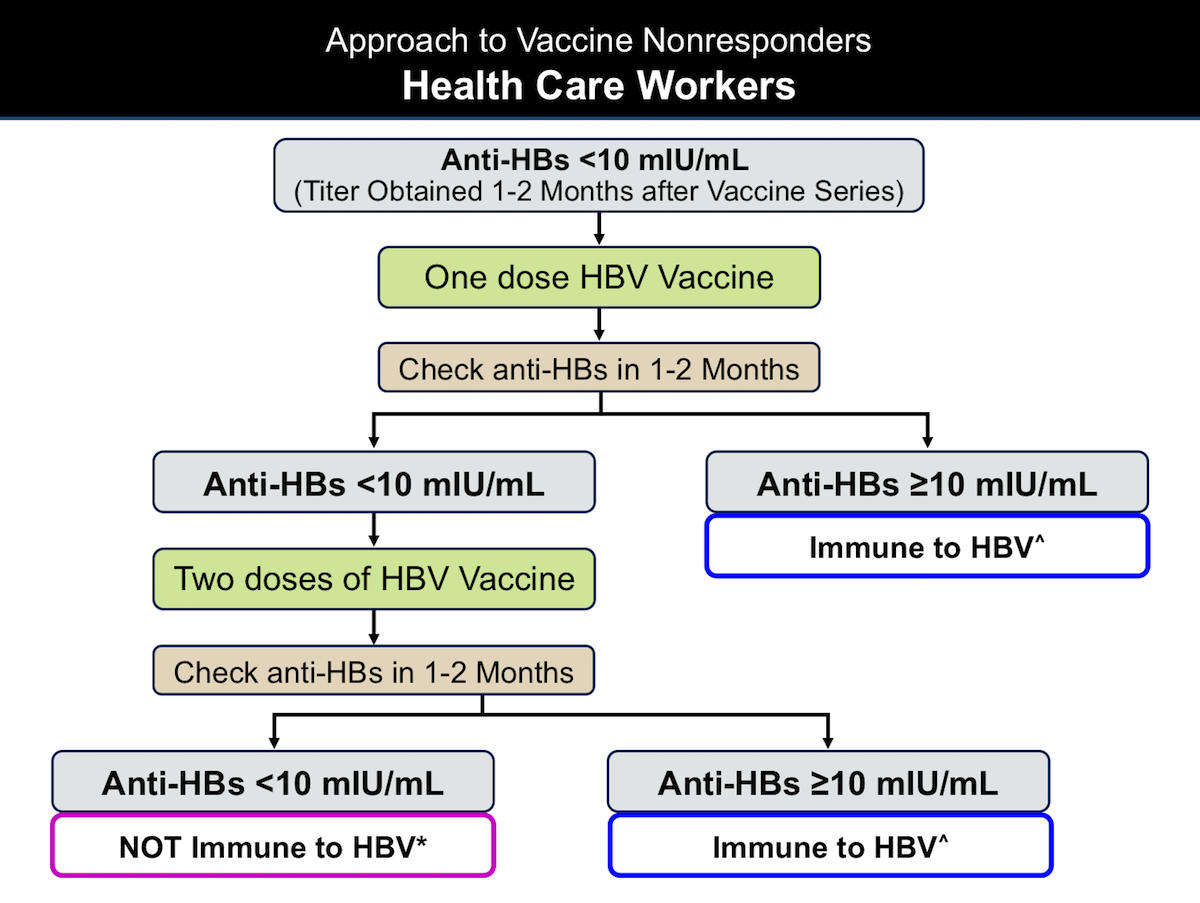
*Health care workers should receive evaluation for all occupational exposures to hepatitis B.
Some experts recommend a more practical alternative strategy for very recently vaccinated health care workers with anti-HBs <10 mIU/mL that consists of giving a second complete series (instead of the one initial dose of hepatitis B vaccine), followed by anti-HBs testing 1–2 months after the final dose.
^For adults, the repeat hepatitis B vaccine series should consist of the high-dose (40 µg per dose) HBsAg given as the 3-dose series for Recombivax-HB or 4 doses for Engerix-B.
*For persons who respond to the repeat vaccine series and have an anti-HBs titer of ≥10 mIU/mL, annual testing for anti-HBs is recommended, with administration of a booster dose of hepatitis B vaccine if the anti-HBs titer is <10 mIU/mL.







Tables
| Groups with Indication for Hepatitis B Vaccination |
| All infants |
| Unvaccinated Children Younger than 19 Years of Age |
| Adults 19 to 59 Years of Age |
|
Adults 60 Years of Age and Older with Risk Factors for Hepatitis B
|
| Adults 60 years of age and older without known risk factors may receive hepatitis B immunization. |
|
Abbreviations: ACIP = Advisory Committee on Immunization Practices; HBsAg = hepatitis B surface antigen; HBV = hepatitis B virus; ALT = alanine aminotransferase; AST = aspartate aminotransferase |
- Schillie S, Vellozzi C, Reingold A, et al. Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2018;67:1-31. [PubMed Abstract]
- Weng MK, Doshani M, Khan MA, et al. Universal Hepatitis B Vaccination in Adults Aged 19-59 Years: Updated Recommendations of the Advisory Committee on Immunization Practices - United States, 2022. MMWR Morb Mortal Wkly Rep. 2022;71:477-83. [PubMed Abstract]
| Single-Antigen Vaccines | Combination Vaccines | |||||||||||
| Age group (years) | Recombivax-HB | Engerix-B | Heplisav-B^ | Pediarix* | Twinrix† | |||||||
| Dose (µg) |
Vol (mL) |
Dose (µg) |
Vol (mL) |
Dose (µg) |
Vol (mL) |
Dose (µg) |
Vol (mL) |
Dose (µg) |
Volume (mL) |
|||
| Standard Dosing | ||||||||||||
| Birth-10 | 5 | 0.5 | 10 | 0.5 | N/A | N/A | 10* | 0.5 | N/A | N/A | ||
| 11-15 | 10§ | 1.0 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | ||
| 11-19 | 5 | 0.5 | 10 | 0.5 | N/A | N/A | N/A | N/A | N/A | N/A | ||
| ≥20 | 10 | 1.0 | 20 | 1.0 | 20 | 0.5 | N/A | N/A | 20† | 1.0 | ||
| Dosing in Hemodialysis Patients and Other Immunocompromised Persons | ||||||||||||
| <20 | 5 | 0.5 | 10 | 0.5 | N/A | N/A | N/A | N/A | N/A | N/A | ||
| ≥20 | 40# | 1.0# | 40 | 2.0 | N/A | N/A | N/A | N/A | N/A | N/A | ||
|
+Note: this table is modified from original to include information on Heplisav-B |
||||||||||||
- Schillie S, Vellozzi C, Reingold A, et al. Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2018;67:1-31. [PubMed Abstract]
| Maternal HBsAg Status | Single-Antigen Vaccine | Single-Antigen + Combination Vaccine^ | |||||
| Dose: Age | Dose: Age | ||||||
| Birth-weight ≥2,000 grams | |||||||
| Positive | Dose 1: At birth (≤12 hours of age) HBIG§: At birth (≤12 hours of age) Dose 2: At age 1-2 months Dose 3: At age 6 months¶ |
Dose 1: At birth (≤12 hours of age) HBIG: At birth (≤12 hours of age) Dose 2: At age 2 months Dose 3: At age 4 months Dose 4: At age 6 months¶ |
|||||
| Unknown* | Dose 1: At birth (≤12 hours) Dose 2: At age 1-2 months Dose 3: At age 6 months¶ |
Dose 1: At birth (≤12 hours) Dose 2: At age 2 months Dose 3: At age 4 months Dose 4: At age 6 months¶ |
|||||
| Negative | Dose 1: At birth (≤24 hours) Dose 2: At age 1-2 months Dose 3: At age 6-18 months¶ |
Dose 1: At birth (≤24 hours) Dose 2: At age 2 months Dose 3: At age 4 months Dose 4: At age 6 months¶ |
|||||
| Birth-weight <2,000 grams | |||||||
| Positive | Dose 1: At birth (≤12 hours of age) HBIG: At birth (≤12 hours of age) Dose 2: At age 1 months Dose 3: At age 2-3 months Dose 4: At age 6 months¶ |
Dose 1: At birth (≤12 hours of age) HBIG: At birth (≤12 hours of age) Dose 2: At age 2 months Dose 3: At age 4 months Dose 4: At age 6 months¶ |
|||||
| Unknown | Dose 1: At birth (≤12 hours of age) HBIG: At birth (≤12 hours of age) Dose 2: At age 1 months Dose 3: At age 2-3 months Dose 4: At age 6 months¶ |
Dose 1: At birth (≤12 hours of age) HBIG: At birth (≤12 hours of age) Dose 2: At age 2 months Dose 3: At age 4 months Dose 4: At age 6 months¶ |
|||||
| Negative | Dose 1: At Hospital Discharge or age 1 month Dose 2: At age 2 months Dose 3: At age 6-18 months¶ |
Dose 1: At Hospital Discharge or age 1 month Dose 2: At age 2 months Dose 3: At age 4 months Dose 4: At age 6 months¶ |
|||||
| Abbreviations: HBsAg = hepatitis B surface antigen; HBIG = hepatitis B immune globulin *Mothers should have blood drawn and tested for HBsAg as soon as possible after admission for delivery; if the mother is found to be HBsAg positive, the infant should receive HBIG as soon as possible but no later than age 7 days. ^Pediarix should not be administered before age 6 weeks. §HBIG should be administered at a separate anatomical site from vaccine. ¶The final dose in the vaccine series should not be administered before age 24 weeks (164 days). |
|||||||
|
|
|
|
|
|
|
|
|
|
|
- Schillie S, Vellozzi C, Reingold A, et al. Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2018;67:1-31. [PubMed Abstract]