Lesson 10. Preventing HBV Perinatal Transmission
Associate Editor
Associate Professor of Medicine
Division of Allergy & Infectious Diseases
University of Washington
Associate Editor
Professor of Medicine
Division of Allergy & Infectious Diseases
University of Washington
Editor-in-Chief
Professor of Medicine
Division of Allergy & Infectious Diseases
University of Washington
Learning Objective Performance Indicators
- Provide universal screening for hepatitis B virus (HBV) infection during pregnancy
- Recognize risks for HBV perinatal transmission in HBsAg-positive mothers
- Treat hepatitis B during pregnancy when indicated
- Summarize risk of HBV perinatal transmission in pregnant women with isolated hepatitis B core antibody
- Apply recommendations for neonatal immunoprophylaxis to prevent perinatal transmission of HBV
Universal Screening for HBV Infection During Pregnancy
Universal screening for hepatitis B virus (HBV) infection is recommended at the first prenatal visit for all pregnant women, regardless of prior hepatitis B vaccination status.[1,2,3] In general, screening should be performed through the serologic detection of hepatitis B surface antigen (HBsAg), hepatitis B surface antibody (anti-HBs), and hepatitis B core antibody (anti-HBc).[2] The use of this triple screening panel allows for the detection of active HBV infection (e.g., positive HBsAg) and identifies pregnant women who are susceptible to HBV and thus candidates for hepatitis B vaccination.[2] Pregnant women who have previously undergone HBV screening with a 3-test panel and do not have any subsequent risk for HBV can be screened using HBsAg alone.[2] In order to ensure postexposure prophylaxis is appropriately given to infants born to HBsAg-positive mothers, a copy of the mother’s hepatitis B test results should be provided to her and the hospital or care facility where she intends to deliver.[4]
- Pregnant Women with Positive HBsAg Screening Test: Expectant mothers who screen positive for HBsAg should undergo additional laboratory testing for a hepatic alanine aminotransferase (ALT) level and a plasma quantitative HBV DNA level to evaluate if HBV treatment is indicated.[1,4]
- Pregnant Women with Negative HBV Screening Tests: Women who screen negative for HBsAg, anti-HBs, and anti-HBc upon enrollment into prenatal care should be offered vaccination against HBV.[1,4,5] Pregnant women can receive any of the commercially available single-antigen hepatitis B vaccines during pregnancy, including Heplisav-B, Engerix-B, or Recombivax-HBV.[4,6]
- Screening for HBV at the Time of Labor and Delivery: Women who were not screened earlier in pregnancy, those with clinical or laboratory evidence of hepatitis, and those with ongoing risk factors for HBV acquisition should have screening for HBV performed at the time of labor and delivery.[4]
Risk of Perinatal HBV Transmission
In the United States, during the year 2021, there were an estimated 17,827 infants born to HBsAg-positive mothers.[7] Although there were only 13 cases of perinatal HBV transmission reported to the CDC in 2022, earlier modeling studies suggest there are approximately 950 cases of perinatally acquired chronic HBV infection in the United States annually.[7,8,9,10] In the absence of HBV postexposure immunoprophylaxis or maternal receipt of antiviral medications, the estimated rate of HBV transmission from an HBsAg-positive mother to her neonate is approximately 40% (range 5 to 90%).[11,12,13,14,15] For HBsAg-positive mothers, three factors prominently impact the risk of perinatal HBV transmission: maternal HBV DNA levels, maternal hepatitis B e antigen (HBeAg) status, and use of hepatitis B immunoprophylaxis for the infant.
- Risk Related to Maternal HBV DNA Levels: The risk of perinatal HBV transmission is significantly increased among mothers who have high plasma HBV DNA levels.[16,17] Studies suggest that even in the presence of timely and effective infant prophylaxis, there is an ongoing risk of HBV perinatal transmission in mothers who have an HBV DNA >200,000 IU/mL.[18,19] In one systematic review and meta-analysis that included 22 studies where infants received birth dose vaccination and HBIG, the incidence of mother to child transmission of HBV was 0.0% when HBV DNA was less than 19,500 IU/mL, but increased steadily with rising DNA levels to 4.3% when maternal HBV DNA was >1,000,000 and 9.6% when maternal DNA was >10,000,000 IU/mL.[19] In an older study from Taiwan, which was conducted from 1972 through 1980, which as prior to the widespread use of immunoprophylaxis for infants, the risk for persistent neonatal infection increased from 3.2% with maternal plasma HBV DNA levels less than 0.005 ng/mL (150,000 IU/mL) to 97.2% with HBV DNA levels greater than 1.4 ng/mL (45,000,000 IU/mL) among 773 HBsAg-positive mothers (Figure 1).[20]
- Risk Related to HBeAg Status: HBeAg positivity also appears to affect risk for perinatal transmission. In the absence of hepatitis B infant immunoprophylaxis or maternal antiviral therapy, an estimated 70 to 90% of infants born to mothers with a positive HBeAg will become infected with HBV, which is markedly higher than the 5-10% of infants born to HBeAg-negative mothers.[6,12,13,21] Similarly, in the Taiwanese study mentioned above, the odds ratio of having an infant with persistent (chronic) HBV infection was 17.6 for HBeAg-positive mothers in comparison to HBeAg-negative mothers.[20]
- Impact of HBV Immunoprophylaxis for the Infant: The risk of perinatal HBV transmission is markedly impacted by the provision of birth dose hepatitis B vaccination and HBIG. In a 2006 Cochrane review, hepatitis B vaccination decreased the risk of perinatal transmission by 72% when compared to placebo or no intervention (relative risk [RR] 0.28 based on four trials).[22] Similarly, the use of HBIG alone reduced the risk of perinatal transmission by 48% when compared to placebo or no intervention (RR 0.52 based on 11 trials). When combined, the use of plasma-derived HBV vaccine and HBIG reduced the occurrence of perinatal HBV infection by 92% (RR 0.08 based on three trials).[22] These results are highlighted in a prospective review of five United States-funded Perinatal Hepatitis B Prevention Programs from 2007 through 2013. In this study, 17,951 infants born to HBsAg-positive mothers were evaluated and information on HBsAg status was available for 51.5% (9,252) of the infants. Overall, 1.1% (100 of the 9,252) infants acquired perinatal HBV. In this cohort, 95% had received the birth dose hepatitis B vaccine and HBIG within 12 hours of birth.[17]
Route and Timing of Perinatal HBV Transmission
The exact mechanism and timing of perinatal HBV transmission remain unclear. It is believed that most infections occur intrapartum, but in utero transmission and postpartum horizontal transmission can also occur.[23] Although HBV DNA and HBsAg have been detected in amniotic fluid, placental cells, and cord blood, the exact timing and mechanisms for transplacental HBV transmission, when it occurs, remain uncertain.[24,25,26,27,28]
- Intrauterine Transmission: The exact timing and mechanism of intrauterine transmission is not clearly known, but the risk would be enhanced with a breach of the placental barrier and mixing of maternal and fetal blood, such as with threatened abortion early in pregnancy or preterm labor.[29,30,31] In a study of infants born to HBsAg-positive mothers in China, 3.7% (15 of 402) were found to be HBsAg positive within 24 hours of birth, which the authors defined as intrauterine transmission.[26] In this study, the main risk factors for intrauterine infection were maternal HBeAg positivity, threatened preterm labor, and the presence of HBV in the placenta, particularly if located in the villous capillary endothelial cells.[26]
- Transmission During Amniocentesis: Perinatal HBV transmission following amniocentesis has been described, and the risk appears to be highest among women with an HBV DNA level of greater than 2,000,000 IU/mL.[32,33]
- Intrapartum/Peripartum Transmission: The greater than 90% efficacy of birth dose vaccination and HBIG in preventing perinatal HBV infection supports the hypothesis that most perinatal infections occur intrapartum.[15,29,34,35] Nevertheless, data on the use of elective cesarean section to reduce mother-to-child transmission are mixed.[29,36,37,38,39] Similarly, there are limited data on the risk of perinatal transmission in the setting of premature rupture of membranes. In one nested case-control study of 141 infant pairs in China, mothers with HBsAg-positive infants were more likely to have experienced premature rupture of membranes prior to birth than those with HBsAg-negative infants.[40] In contrast to these findings, a Korean study of 144 children born to HBsAg-positive mothers reported no correlation between premature rupture of membranes and increased risk for perinatal transmission.[41]
- Transmission via Breast Milk: Transmission of HBV through breast milk is not a major concern, as several studies have suggested very low rates of transmission via breastfeeding, despite HBV being present in colostrum.[39,42,43,44] In a recent population-based cohort study from Korea, the odds of perinatal transmission were lower among infants who were breastfed as opposed to those who received formula, providing further evidence that breastfeeding is safe in HBsAg-positive mothers.[39] Similar studies performed before the routine use of neonatal prophylaxis also suggested a limited risk of vertical transmission among breastfeeding mothers.[43,44]
Management of Women with Chronic HBV in Pregnancy
Antiviral therapy to treat HBV in pregnant women can have two potential benefits: (1) prevent perinatal transmission of HBV, and (2) treat chronic HBV in the mother, if indicated.[45] The 2025 AASLD/IDSA HBV Treatment Guideline recommends the use of the nucleotide reverse transcriptase inhibitors tenofovir DF or tenofovir alafenamide as the preferred antiviral agents to treat HBV in pregnant women.[46,47,48,49,50,51] The following summary outlines the general approach for the potential use of antiviral therapy in HBsAg-positive pregnant women.
Recommended Antiviral Regimens to Treat HBV During Pregnancy
Historically, tenofovir DF has been the preferred medication for treatment of HBV during pregnancy, primarily due to excellent potency, high barrier to resistance, a known good safety profile in pregnancy, and proven efficacy in preventing perinatal transmission in mothers with HBV DNA levels greater than 200,000 IU/mL (Figure 2).[1,52,53,54] There is, however, robust evidence that now supports the safety and efficacy of tenofovir alafenamide both for the treatment of HBV during pregnancy and for the prevention of perinatal transmission.[46,47,48,49,50,55] Therefore, either oral tenofovir DF or oral tenofovir alafenamide is a suitable option to treat hepatitis B in pregnant women, and both are recommended in the 2025 AASLD/IDSA HBV Treatment Guideline.[51] The recommended dose of tenofovir DF is 300 mg daily. Prior to starting tenofovir DF, the following baseline laboratory studies should be performed: serum creatinine, estimated creatinine clearance, urine glucose, and urine protein. The dose of tenofovir DF must be adjusted and reduced in persons who have a creatinine clearance less than 50 mL/min. The recommended dose of tenofovir alafenamide is 25 mg daily; this medication is not recommended for use in persons with a creatinine clearance less than 15 mL/min but requires no dose adjustment for a creatinine clearance of 15 mL/min or greater.
HBsAg-Positive Women Not on Antiviral Therapy at the Time of Pregnancy
- Indications for HBV Therapy to Prevent Perinatal HBV Transmission: For HBsAg-positive women who are not on HBV therapy at the time they become pregnant, the main indication for initiating HBV to prevent perinatal HBV transmission is a maternal HBV DNA level greater than 200,000 IU/mL at any time point in pregnancy.[4,51] This recommendation is based on data that suggest (1) perinatal HBV infections can occur even when infants receive appropriate doses of hepatitis B vaccination and HBIG, with most of these cases involving mothers with high plasma HBV DNA levels, and (2) the use of antiviral therapy in the third trimester can significantly reduce perinatal HBV transmission.[1,51,52,56,57] In mothers with an HBV DNA level greater than 200,000 IU/mL who are not otherwise on HBV antiviral therapy, the 2025 AASLD/IDSA HBV Treatment Guideline recommends initiating HBV therapy at 28 weeks’ gestation with either tenofovir DF or tenofovir alafenamide.[51] In settings where infant HBIG is not available, HBV antiviral prophylaxis with tenofovir DF or tenofovir alafenamide should be started at 16 weeks’ gestation in mothers with an HBV DNA greater than 200,000 IU/mL.[51] This earlier start is based off data from a recent randomized controlled trial that found similar rates of perinatal HBV transmission with two different strategies: (1) the mother started tenofovir DF at 16 weeks' gestation and the infant received a birth-dose hepatitis B vaccination versus (2) the mother started tenofovir DF at 28 weeks’ gestation and the infant received a birth-dose vaccination and HBIG.[58]
- Indications for HBV Therapy for Maternal Benefit: All HBsAg-positive women who are not on HBV therapy at the time they become pregnant should undergo evaluation to determine if they have an indication to start therapy based on treatment guidelines for persons with chronic HBV.[51,59,60] We recommend initiating HBV therapy for the purposes of maternal benefit for pregnant women who have (1) cirrhosis and/or (2) the presence of elevated HBV DNA (2,000 IU/mL or greater) and elevated ALT (greater than 25 U/mL). In addition, as noted above, pregnant women who have an HBV DNA level greater than 200,000 IU/mL should initiate antiviral treatment regardless of ALT levels at 28 weeks’ gestation, or at 16 weeks’ gestation if HBIG will not available for their infant.[4,51]
- Monitoring Women Who Do Not Meet Criteria for Treatment: For pregnant women who do not meet criteria for antiviral therapy, some experts recommend monitoring ALT levels every 3 months during pregnancy and for at least 6 months postpartum, primarily because of possible hepatic flares that can occur as a result of pregnancy-associated immunologic changes. In addition, HBV DNA should be checked at 26 to 28 weeks’ gestation (and concurrent with any elevation of ALT) to determine the need for antiviral initiation in the third trimester (starting at 28 weeks’ gestation) to prevent perinatal transmission.[1,4,51,61]
- Duration of Antiviral Therapy for Pregnant Women: Antiviral therapy initiated purely for the prevention of mother-to-child transmission of HBV can be discontinued at delivery. In this situation, however, women should undergo postpartum lab monitoring at least every 3 months and for at least 6 months to assess for hepatitis flares and seroconversion; some experts recommend more intensive monitoring with ALT and HBV DNA at 1, 3, and 6 months postpartum.[1,53] Postpartum HBV flares are common, especially among HBeAg-positive women who stop oral antiviral therapy, but there are no formal recommendations to extend oral antiviral therapy after delivery in women who do not otherwise meet hepatitis B treatment criteria.[51,62,63] Women who have an indication for HBV treatment other than for preventing perinatal HBV transmission should continue on therapy indefinitely and follow the same treatment guidelines for monitoring and potentially discontinuing therapy as for all individuals receiving chronic treatment for HBV.[1,51,61]
HBsAg-Positive Women on Hepatitis B Therapy at the Time of Pregnancy
Women who are HBsAg positive and become pregnant while taking antiviral therapy to treat HBV should discuss the pros and cons of continuing therapy with their health care provider. The 2025 AASLD/IDSA HBV Treatment Guideline recommends continuing antiviral HBV treatment in this situation, both for the mother’s benefit (reducing the risk of a hepatitis flare during pregnancy) and for decreasing the risk of perinatal HBV transmission.[51] Tenofovir DF or tenofovir alafenamide are the medications of choice for HBV treatment during pregnancy, and available data suggest both are safe for use during pregnancy and for breastfeeding.[46,47,49,51,52,64] For pregnant women who are going to continue receiving HBV treatment but are taking a regimen other than tenofovir DF or tenofovir alafenamide, it is important they promptly switch the antiviral therapy to either tenofovir DF or tenofovir alafenamide, owing to their favorable safety profile in pregnancy, high barrier to resistance, and established efficacy in preventing perinatal HBV transmission.[46,48,49,52] If the pregnant woman and the medical provider choose to continue entecavir for hepatitis B treatment during the pregnancy, she should consider being enrolled in the Antiviral Pregnancy Registry, which collects deidentified data on drug safety and pregnancy outcomes. Similar treatment endpoints should also be used for pregnant women as for nonpregnant women with chronic HBV.
Considerations at the Time of Labor and Delivery
There is no clear evidence of reduced perinatal HBV transmission among women who deliver via cesarean section, and as such, the [1] guidelines recommend against the routine use of elective cesarean section in HBsAg-positive mothers.[1] Similarly, owing to limited data on the risk of perinatal transmission in the setting of premature rupture of membranes, recommendations for the management of HBsAg-positive women who have premature rupture of membranes are the same as for HBsAg-negative women who have premature rupture of membranes. In addition, there are no recommendations to give extra doses or additional antiviral medications to mothers during labor and delivery.
Considerations Regarding Amniocentesis
Perinatal HBV transmission following amniocentesis has been described, particularly among pregnant women with high plasma HBV DNA levels (greater than 2,000,000 IU/mL).[32] The 2025 AASLD/IDSA HBV Treatment Guideline recommends consideration of antiviral therapy initiation early in pregnancy in women with HBV DNA levels greater than 2,000,000 IU/mL when invasive procedures are anticipated; although the exact timing of when to initiate antiviral therapy is not specified.[51]
Management of Pregnant Women with Isolated Anti-HBc
Potential Causes of Isolated Anti-HBc
The detection of hepatitis B core antibody (anti-HBc) indicates exposure to HBV and can be present in active and resolved infections. Specifically, detection of an isolated anti-HBc can be seen in four distinct clinical scenarios: (1) window phase of acute infection (prior to development of anti-HBs and following loss of HBsAg); (2) resolved HBV infection with waning anti-HBs; (3) occult HBV with loss of HBsAg but positive HBV DNA; and (4) a rare false-positive test. In clinical practice, the presence of an isolated anti-HBc most often reflects resolved HBV infection with waning anti-HBs over time.
Occult HBV Infection in Persons with Isolated Anti-HBc
Although occult HBV is a consideration in persons with an isolated anti-HBc, the prevalence of occult HBV varies by population and geographic region. In addition, most studies do not evaluate the prevalence of occult HBV strictly within persons who have an isolated anti-HBc but rather more broadly in persons who are HBsAg negative and HBV DNA positive, regardless of anti-HBc or anti-HBs status.
- In a global systematic review and meta-analysis that evaluated the prevalence of occult HBV in blood donors, 6.2% of individuals with a negative HBsAg and positive anti-HBc were found to have occult HBV, with the prevalence being generally higher in low-income countries.[65] It is important to note this study did not systematically evaluate anti-HBs status, so it does not reflect the prevalence of occult HBV among those with a strictly isolated anti-HBc profile, but rather reflects the prevalence of occult HBV in the broader population of persons who are HBsAg negative, regardless of other serologic markers.[65]
- In a similar global systematic review and meta-analysis that evaluated the prevalence of occult HBV in HBsAg negative blood donors, regardless of anti-HBc status, the overall prevalence of occult HBV was 0.06% (0.00-0.26) in low-endemicity countries, 0.12% (0.04-0.23) in intermediate-endemicity countries, and 0.98% (0.44-1.72) in high-endemicity countries.[66]
- In the United States, NHANES survey data from 2001 through 2018 suggest the prevalence of occult HBV among persons with isolated anti-HBc is between 1.7% and 4.0%, although these estimates are subject to the limitations of NHANES data, which does not include incarcerated or unhoused populations.[67]
- There are no published estimates of the prevalence of occult HBV in pregnant women in the United States, but data from other geographic regions suggests that the prevalence is likely low.
- In a large Chinese study that evaluated antenatal screening data from 2015 through 2022, the prevalence of occult HBV was 0% among women with an isolated anti-HBc.[68]
- In a study evaluating the HBV serologic profiles among pregnant women in Iran, 2.9% (41 of 1,425) were found to be anti-HBc positive, of whom 2.4% (1 of 41) were HBsAg negative but had detectable HBV DNA; anti-HBs status was not evaluated in this study.[69]
- Other studies evaluating the prevalence of occult HBV during pregnancy in Russia and Nigeria report a prevalence of 2.8% and 2.5%, respectively; these studies, however, do not specify the presence or absence of an isolated anti-HBc.[70,71]
Perinatal HBV Transmission Risk with Occult HBV
When present, occult HBV is typically associated with low HBV viral loads and, therefore, a lower risk of transmission. Studies suggest that HBV DNA levels in occult infection are usually less than 200 IU/mL and often close to the lower limits of assay detection.[72,73,74,75] In a cross-sectional study from Nigeria, the average HBV DNA level among pregnant women with occult HBV was 2.30 log IU/mL (2.19-3.00), compared to 4.84 log IU/mL (4.00-9.14) among pregnant women with overt HBV.[71]
Management of Pregnant Women with Isolated Anti-HBc
There are no specific guidelines for the management of pregnant women with isolated anti-HBc, and most women with this serologic profile will have resolved HBV infection with waning anti-HBs. Pregnant women with an isolated anti-HBc should be counseled about their history of HBV infection and potential risk for reactivation, particularly if they are receiving any immunosuppressive medications or have an immunosuppressive condition. In addition, follow-up of isolated anti-HBc results with HBV DNA testing should strongly be considered in all pregnant women to identify the presence of occult HBV DNA and to further guide management decisions for both the pregnant woman and the infant. The following recommendations are based on results of the HBV DNA testing of the mother.
- If the mother has an undetectable HBV DNA result, the infant should be given a hepatitis B birth dose vaccination followed by the complete vaccine series, as per standard guidance.[4] The mother should receive further evaluation, counseling, and follow-up related to hepatitis B reactivation risk.
- If the mother has a positive (detectable) HBV DNA result, the infant should receive hepatitis B postexposure prophylaxis that is the same as given to infants born to women with positive HBsAg, including a single 0.5 mL dose of hepatitis B immune globulin and a dose of single antigen hepatitis B vaccine, both within 12-hours of birth. Subsequently, completion of the hepatitis B vaccine series should occur, with the number of doses for the infant based on birth weight. These infants should have HBV serologic testing at approximately 9 to 12 months of age to include both anti-HBs and HBsAg.[4] Mothers who are identified with detectable HBV DNA should be referred to an expert in the management of viral hepatitis. These mothers should be managed during pregnancy according to guidelines for pregnant women who are HBsAg positive, including HBV treatment initiation at 28–32 weeks of gestation if the HBV DNA level is greater than 200,000 IU/mL at any time point in the pregnancy.[51]
Management of Acute HBV in Pregnancy
Impact of Acute Hepatitis B in Pregnancy
Acute hepatitis B infection during pregnancy is typically mild (for the mother) and nonteratogenic, but it may confer a higher risk for low birth weight and prematurity.[76,77] Similarly, mothers with acute HBV during pregnancy may be more likely to progress to chronic infection, with one study from China suggesting that pregnant women with acute HBV had a relative risk of 4.6 for the development of chronic infection when compared with nonpregnant women controls.[78] Acquisition of acute HBV near the time of delivery poses the highest risk for perinatal transmission; therefore, women with ongoing risk factors for HBV acquisition should undergo repeat HBV screening near the time of delivery.[4,76,77]
Treatment of Acute Hepatitis B During Pregnancy
Treatment of acute hepatitis B infection during pregnancy should be considered when the mother has: (1) a plasma HBV DNA level of greater than 200,000 IU/mL at any time during the third trimester, (2) severe, protracted hepatitis (increase in international normalized ratio [INR] and jaundice persisting for greater than 4 weeks), and/or (3) acute fulminant liver failure.[1,79] Management of women with protracted hepatitis during pregnancy or with fulminant liver failure should include the involvement of experts, ideally both a hepatologist and an obstetrician who have experience managing this complicated issue.
Safety of Antivirals During Pregnancy
No antiviral medications have been FDA-approved for the treatment of chronic hepatitis B during pregnancy, owing to a lack of large-scale studies evaluating antiviral safety in pregnant women with HBV monoinfection. There are, however, large-scale studies with tenofovir DF in pregnant women with HIV that suggest it is safe for use during pregnancy.[80,81] In addition, newer evidence supports the safety and efficacy of tenofovir alafenamide in pregnancy, and smaller studies evaluating tenofovir DF and tenofovir alafenamide for the prevention of mother-to-child transmission in HBV have shown no evidence of adverse effects on the infant.[34,46,48,50,52,56] The Antiretroviral Pregnancy Registry includes self-reported adverse effects of antivirals used during pregnancy for the treatment of HIV and/or HBV.[82] The following summarizes pregnancy-related information for the three preferred oral antiviral agents to treat HBV. Interferon and peginterferon are contraindicated for use during pregnancy and thus will not be discussed further here.
- Entecavir: The nucleoside analogue entecavir is highly active against HBV. It is not used in the treatment of HIV, and therefore, limited data exist on its use during pregnancy. Although animal studies in rats and rabbits revealed no signs of embryo-fetal toxicity, no well-controlled studies have been done in pregnant women. As such, the use of entecavir is not recommended during pregnancy.
- Tenofovir alafenamide: Tenofovir alafenamide is a nucleotide analogue that has been used to treat HBV and, in combination with other antiretroviral medications, to treat HIV. Evidence supports the safety and efficacy for tenofovir alafenamide in pregnant women, and it is now recommended for use in pregnancy by the Perinatal HIV Guidelines, the 2025 EASL Hepatitis B Guidelines, and the 2025 AASLD/IDSA HBV Treatment Guideline.[46,47,49,50,51,64,83] Tenofovir alafenamide exposure in breastmilk has been evaluated in pharmacokinetic studies of women living with HIV, and in one study of women with HBV. Although tenofovir concentrations in breast milk have been found to be higher in women taking tenofovir alafenamide, as compared to tenofovir DF, the relative infant exposure remains very low.[84,85,86]
- Tenofovir DF: With the nucleotide analogue tenofovir DF, longitudinal human data have not shown an increased risk for teratogenicity among babies born to mothers who took tenofovir DF during pregnancy, although most of these women were taking tenofovir DF for HIV therapy.[87,88] In comparison to an estimated 3% rate of birth defects in the general United States population, the Antiretroviral Pregnancy Registry has found a 2.4% risk of birth defects in babies born to mothers who took any tenofovir DF-containing regimen during the first trimester and a 2.3% risk of birth defects when mothers took a tenofovir DF-containing regimen during the second and third trimester.[82] Despite some concern regarding the effect of in utero tenofovir DF exposure on bone health, a recent study of children born to mothers with HIV found no difference in length of head circumference at 2 years of age for children exposed to tenofovir DF in utero compared to children not exposed to tenofovir DF.[89,90] The safety of tenofovir DF is also well established in the setting of lactation, and treatment is safe to continue in the postpartum period while the mother is breastfeeding.
Hepatitis B Flares During Pregnancy and in the Postpartum Period
Although women with chronic HBV infection typically tolerate the infection well during pregnancy, the relative immunosuppressant state of pregnancy often causes hepatitis flares, with even greater risk in the postpartum period.[62,91] In a prospective study of predominantly untreated, pregnant women with chronic HBV in Australia, 25% (27 of 108) of the women for whom postpartum labs were available had evidence of a postpartum hepatitis flare based on increases in ALT levels.[91] By comparison, only 1.6% (2 of 126) of women experienced a hepatitis flare during pregnancy in this cohort.[91] Flares during pregnancy and in the postpartum period are often mild, but rare cases of fulminant liver failure have been described.[92,93] In women with chronic hepatitis B, the risk for postpartum HBV flares is common regardless of receipt of antiviral therapy during pregnancy and even when treatment is extended for at least 4 weeks after birth.[63] The 2025 AASLD/IDSA HBV Treatment Guideline recommends women who discontinue hepatitis B antiviral treatment after birth of their child should have monitoring for hepatitis flares by checking HBV DNA and ALT levels and every 1–3 months for up to 6 months.[51] Antiviral treatment should be restarted there is laboratory evidence of a significant hepatitis flare (ALT level greater than 5 times the upper limit of normal).[51]
Management of Neonates Born to HBsAg-Positive Mothers
Recommendations for neonatal immunoprophylaxis to prevent perinatal transmission of HBV differ depending on the HBsAg status of the mother and the birth weight of the infant. When giving the birth dose hepatitis B vaccination and any doses before age 6 weeks, the single-antigen (monovalent) hepatitis B vaccine should be used. For infants 6 weeks of age and older, the combined vaccine (Pediarix) can be substituted for the single-antigen hepatitis B vaccines (Engerix-B or Recombivax-HB). If, however, Pediarix is used, the full three-shot series of Pediarix must be completed, regardless of receipt of birth dose vaccination or maternal HBsAg status.[4] The following reflects recommendations from the 2018 CDC Advisory Committee on Immunization Practices (ACIP) guidance.[4]
Infants Born to HBsAg-Positive Mothers
All infants born to HBsAg-positive women, or women with other evidence of chronic HBV infection (e.g., positive HBV DNA, positive HBeAg, or known history of chronic HBV infection) should receive an intramuscular dose of single-antigen hepatitis B vaccine and one dose of intramuscular HBIG (0.5 mL), both within 12 hours of birth. The hepatitis B vaccine and HBIG should be given regardless of birth weight or maternal antiviral therapy, and the injections should be at different sites on the body. The vaccine schedule and doses depend on the infant’s weight.[4]
- Infants Weighing at Least 2,000 Grams: Infants weighing at least 2,000 grams (4.4 pounds) should receive a second hepatitis B vaccine dose at 1 to 2 months of age and a third dose at 6 months of age; the final vaccine dose should not be administered before age 24 weeks (164 days).
- Infants Weighing Less than 2,000 Grams: For infants weighing less than 2,000 grams (4.4 pounds) at birth, the birth dose vaccine should not be counted towards their three-shot series due to possible decreased immunogenicity in these low-birth-weight infants. As such, they should receive an additional 3 doses of vaccine, given at 1, 2 to 3, and 6 months of age (for a total of 4 doses); the final vaccine dose should not be administered before age 24 weeks (164 days).
- Follow-Up Serologic Testing: After completion of the HBV vaccine series, all infants born to HBsAg-positive mothers should receive HBV serologic testing at approximately 9 to 12 months of age (making sure this is done at least 1 month after the final hepatitis B vaccine series dose and at least 9 months after HBIG has been given). Testing for anti-HBc is not recommended since passive transfer of maternal anti-HBc may persist for 24 months. Infants who test HBsAg negative and have an anti-HBs level of 10 mIU/mL or greater are considered immune to HBV.
- Infants who test HBsAg positive should be referred for appropriate follow-up.
- The preferred approach for HBsAg-negative infants who have an anti-HBs level of less than 10 mIU/mL is to first give one additional dose of HBV vaccine, followed by repeat serologic testing in 1 to 2 months after this dose (Figure 3). If anti-HBs levels remain below 10 mIU/mL after a single repeat dose, infants should receive an additional two doses of vaccine to complete another three-dose series. This should again be followed by repeat serologic testing in 1 to 2 months, but if the child has not obtained immunity to HBV at this point, subsequent doses of vaccine are unlikely to provide additional benefit; these children are considered at risk of acquiring HBV, and prevention measures should be used.
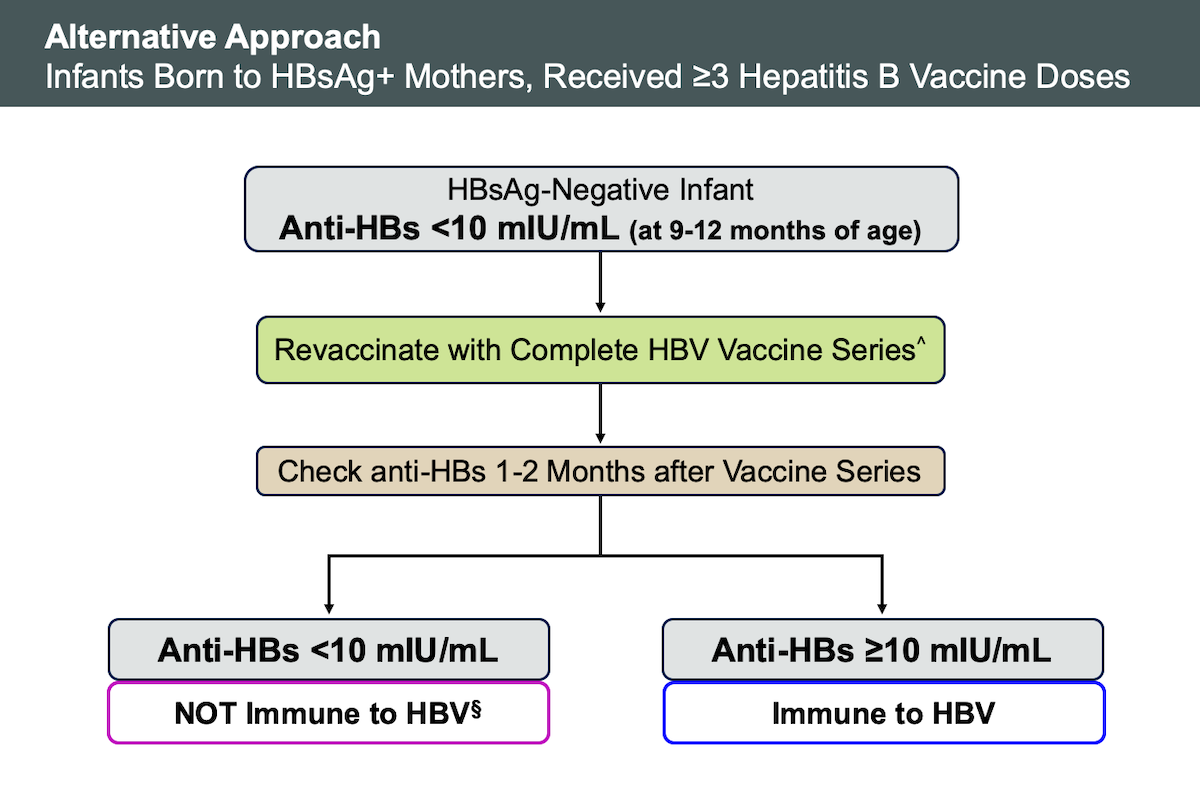
- The alternative approach for infants with an anti-HBs level less than 10 mIU/mL at 9 to 12 months of age is to revaccinate with 3 doses of the HBV vaccine and then repeat serologic testing 1 to 2 months after the last vaccine dose (Figure 4).
Infants Born to Mothers of Unknown HBsAg Status
Women without documentation of prior HBsAg testing should be screened at the time of delivery. The management in this situation is stratified based on the birth weight of the infant and the results of the mother’s HBsAg test.[4]
- Infants Weighing at Least 2,000 Grams: While maternal HBsAg test results are pending, infants weighing 2,000 grams or more should receive the single-antigen hepatitis B vaccine within 12 hours of birth; administration of HBIG is not recommended in this situation. If the mother’s HBsAg test result is known later and is positive, then HBIG should be administered as soon as possible, but no later than 7 days after birth. Regardless of the mother’s test result, the infant should complete a standard three-dose hepatitis B vaccination series, with the remaining additional doses at 1 to 2 months and 6 months; the final vaccine dose should not be administered before age 24 weeks (164 days). If the mother’s HBsAg test result returns and is negative, the infant should not receive HBIG. If the HBsAg status of the mother remains unknown (e.g., in the case of confidential adoption), the infant should complete the standard three-shot hepatitis B vaccine series according to the recommended schedule for infants born to HBsAg-positive mothers; in this scenario, HBIG is not indicated.
- Infants Weighing Less than 2,000 Grams: Due to decreased immunogenicity of the hepatitis B vaccine among infants with low birth weight, infants weighing less than 2,000 grams should receive the single-antigen vaccine in addition to HBIG (administered at different sites on the body) if the mother’s HBsAg status cannot be determined within 12 hours of birth. If the mother’s HBsAg test is positive, or if the mother’s HBsAg status remains unknown, low-birth-weight infants should complete a four-shot vaccination series as described in the section above on infants born to HBsAg-positive mothers. If the mother is ultimately found to be HBsAg negative, then infants less than 2,000 grams need only complete three doses of hepatitis B vaccine at the time of birth and subsequently at 2 months and 6 to 18 months; the final vaccine dose should not be administered before age 24 weeks (164 days).
- Follow-Up Serologic Testing: If the mother's HBsAg test is negative, then postvaccination serologic testing for the infant is not recommended. If the mother’s HBsAg testing is positive, or the mother’s HBsAg status remains unknown, the infant should receive HBV serologic testing at 9 to 12 months of age (making sure this is done at least 1 month after the final hepatitis B vaccine series dose and at least 9 months after HBIG has been given). Infants who test HBsAg negative and have an anti-HBs level of 10 mIU/mL or greater are considered immune to HBV. Infants with an anti-HBs of less than 10 mIU/mL are not immune and need further immunizations as outlined above for infants born to HBsAg-positive mothers.
Infants Born to HBsAg-Negative Mothers
The management of infants born to HBsAg-negative mothers varies slightly based on the infant’s weight.[4]
- Infants Weighing at Least 2,000 Grams: All infants weighing 2,000 grams or more born to HBsAg-negative mothers should receive their first HBV vaccine within 24 hours of birth. They should subsequently complete their hepatitis B vaccine series, with the second dose at 1 to 2 months of age and the third dose at 6 to 18 months of age; the final vaccine dose should not be administered before age 24 weeks (164 days).
- Infants Weighing Less than 2,000 Grams: Infants weighing less than 2,000 grams at birth should receive their first hepatitis B vaccine dose at the time of hospital discharge or at chronological age 1 month, whichever comes first, even if they still weigh less than 2,000 grams. These infants should complete the remaining doses of hepatitis B vaccine, with the second dose at age 2 months (making sure the second dose is given at least 1 month after the first dose) and the third dose at age 6 to 18 months (making sure the third dose is given at least 8 weeks after the second dose and at least 16 weeks after the first dose); the final vaccine dose should not be administered before age 24 weeks (164 days).
- Follow-Up Serologic Testing: There are no recommendations to perform routine follow-up serologic testing in infants born to HBsAg-negative mothers.
Efficacy of Immunoprophylaxis
Several studies and meta-analyses support the efficacy of birth dose HBV vaccination and HBIG in preventing vertical transmission of hepatitis B. When compared to no intervention, a 2006 Cochrane review found that HBV vaccine plus HBIG dramatically decreased the risk of perinatal transmission, with a relative risk of 0.08.[22] Similarly, several prospective studies have shown high efficacy rates for immunoprophylaxis in infants born to HBsAg-positive mothers, with less than 2% of exposed infants developing HBV infection when receiving both the HBIG and hepatitis B vaccine.[17,94] The same Cochrane review found that HBIG plus hepatitis B vaccine significantly decreased the rate of perinatal transmission when compared to hepatitis B vaccination alone (relative risk, 0.54).[22]
Other Impacts of Maternal HBV on Infants
The effect of chronic maternal HBV infection on other noninfectious neonatal outcomes is uncertain. In a large study comparing 824 HBsAg-positive pregnant women with 6,281 HBsAg-negative pregnant women, the investigators found no difference in incidence of preterm birth, premature rupture of membranes, low birth weight, neonatal jaundice, fetal distress, perinatal asphyxia, congenital abnormalities, gastrointestinal tract abnormalities, or perinatal mortality.[95] A similar study from Germany found no difference in adverse pregnancy outcomes among 39 HBsAg-positive women when compared to 8,154 HBsAg-negative women.[96] Several other reports, however, have cited higher rates of preterm birth, lower birth weight, congenital malformations, and lower Apgar scores among infants born to HBsAg-positive mothers.[97,98,99,100]
Breastfeeding in HBsAg-Positive Mothers
Risk of HBV Transmission via Breastfeeding
Transmission of HBV through breast milk is not a significant source of perinatal HBV transmission, and there is no contraindication to breastfeeding in mothers with HBV monoinfection.[1,42,43,44] In the United States, however, women who have HBV and HIV coinfection should not breastfeed, due to the substantial risk of HIV transmission during breastfeeding.
Safety of Antiviral Medications During Breastfeeding
There are insufficient long-term safety data on breastfeeding among mothers receiving antiviral therapy for HBV treatment. Although drug labels recommend against breastfeeding while taking tenofovir DF, this antiviral medication is unlikely to pose significant harm to breastfeeding infants.[1,53] Although limited data are available in women with HBV monoinfection, studies done in women with HIV living in resource-limited settings support the safety of tenofovir DF during breastfeeding and suggest that drug concentrations in breast milk are quite low.[53,101,102,103]. Similar pharmacokinetic studies show that tenofovir alafenamide concentrations are low in breast milk, and infant exposure to tenofovir alafenamide is felt to be negligible.[84,85,86]
Recommendation for Breastfeeding in Women with Chronic HBV
The 2025 AASLD/IDSA HBV Treatment Guideline states that breastfeeding is not contraindicated in HBsAg-positive mothers and breastfeeding women who require antiviral therapy for treatment of hepatitis B should receive tenofovir DF or tenofovir alafenamide.[51]
Summary Points
- All pregnant women should undergo serologic screening for hepatitis B infection at their first prenatal visit, regardless of prior hepatitis B vaccination status.
- The overall rate of HBV transmission from an HBsAg-positive mother to her neonate is approximately 40% in the absence of HBV postexposure immunoprophylaxis or maternal receipt of antiviral medication. Increased risk of perinatal HBV transmission is associated with high maternal plasma HBV DNA levels, maternal HBeAg-positive status, and lack of appropriate immunoprophylaxis for babies.
- The exact mechanisms and timing of perinatal HBV transmission are unclear, but given the greater than 90% efficacy of birth dose vaccination and HBIG, most infections are believed to occur intrapartum.
- Indications for initiation of HBV treatment are generally the same in pregnant and nonpregnant women, except that pregnant women with an HBV DNA level of greater than 200,000 IU/mL (at any time point during the pregnancy) should initiate antiviral treatment, ideally during weeks 28 to 32 of gestation, to prevent perinatal transmission.
- When antiviral therapy for hepatitis B is indicated in pregnancy, tenofovir DF or tenofovir alafenamide are preferred due to their potency, high barrier to resistance, known safety profile in pregnancy, and proven efficacy in preventing perinatal transmission of HBV in pregnant women who have an HBV DNA level greater than 200,000 IU/mL at any time point during pregnancy.
- Women with chronic HBV who are not on antiviral therapy are at risk of hepatitis B flares in the postpartum setting and should undergo laboratory assessment with ALT and HBV DNA level every 1–3 months for at least 6 months after pregnancy. Women with chronic HBV who are initiated on antiviral therapy primarily for the prevention of HBV transmission can discontinue therapy as early as delivery but should undergo close monitoring given the risk of HBV reactivation or flare in the setting of tenofovir withdrawal.
- In general, HBsAg-positive women who become pregnant while on therapy should continue antiviral HBV treatment. If they are on a drug other than tenofovir DF or tenofovir alafenamide, they should promptly switch to tenofovir DF or tenofovir alafenamide, given the known safety profile of these medications in pregnancy.
- Acute HBV infection during pregnancy is typically mild and nonteratogenic, but it may confer a higher risk for low birth weight and prematurity. Treatment is only indicated if the mother’s HBV DNA level is greater than 200,000 IU/mL (at any time point in the pregnancy) or in the setting of protracted and/or fulminant hepatitis.
- All infants born to HBsAg-positive women should receive an intramuscular dose of single-antigen hepatitis B vaccine and one dose of intramuscular HBIG (0.5 mL), both within 12 hours of birth. These should be given regardless of birth weight or maternal antiviral therapy.
- After completion of the HBV vaccine series, all infants born to HBsAg-positive mothers should receive HBV serologic testing at approximately 9 to 12 months of age, making sure this is done at least 1 month after the final hepatitis B vaccine series dose and at least 9 months after HBIG has been given.
Citations
- 1.Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67:1560-99.[PubMed Abstract] -
- 2.Conners EE, Panagiotakopoulos L, Hofmeister MG, et al. Screening and Testing for Hepatitis B Virus Infection: CDC Recommendations - United States, 2023. MMWR Recomm Rep. 2023;72:1-25.[PubMed Abstract] -
- 3.US Preventive Services Task Force, Owens DK, Davidson KW, et al. Screening for Hepatitis B Virus Infection in Pregnant Women: US Preventive Services Task Force Reaffirmation Recommendation Statement. JAMA. 2019;322:349-54.[PubMed Abstract] -
- 4.Schillie S, Vellozzi C, Reingold A, et al. Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2018;67:1-31.[PubMed Abstract] -
- 5.Weng MK, Doshani M, Khan MA, et al. Universal Hepatitis B Vaccination in Adults Aged 19-59 Years: Updated Recommendations of the Advisory Committee on Immunization Practices - United States, 2022. MMWR Morb Mortal Wkly Rep. 2022;71:477-83.[PubMed Abstract] -
- 6.Sandul AL, Rapposelli K, Nyendak M, Kim M. Updated Recommendation for Universal Hepatitis B Vaccination in Adults Aged 19-59 Years - United States, 2024. MMWR Morb Mortal Wkly Rep. 2024;73:1106.[PubMed Abstract] -
- 7.Centers for Disease Control and Prevention (CDC). Clinical Overview of Perinatal Hepatitis B.Infection Rates and Trends.[CDC] -
- 8.Committee on Infectious Diseases; Committee on Fetus and Newborn. Elimination of Perinatal Hepatitis B: Providing the First Vaccine Dose Within 24 Hours of Birth. Pediatrics. 2017;140.pii: e20171870.[PubMed Abstract] -
- 9.Ko SC, Fan L, Smith EA, Fenlon N, Koneru AK, Murphy TV. Estimated Annual Perinatal Hepatitis B Virus Infections in the United States, 2000-2009. J Pediatric Infect Dis Soc. 2016;5:114-21.[PubMed Abstract] -
- 10.Centers for Disease Control and Prevention (CDC). 2023 Viral Hepatitis Surveillance Report—Hepatitis B. Published April 15, 2025.[CDC] -
- 11.Beasley RP, Hwang LY, Lee GC, et al. Prevention of perinatally transmitted hepatitis B virus infections with hepatitis B immune globulin and hepatitis B vaccine. Lancet. 1983;2:1099-102.[PubMed Abstract] -
- 12.Mast EE, Margolis HS, Fiore AE, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP) part 1: immunization of infants, children, and adolescents. MMWR Recomm Rep. 2005;54:1-31.[PubMed Abstract] -
- 13.Silverman NS. Hepatitis B Screening in Pregnant Women: A Perspective on the New USPSTF Recommendations. JAMA. 2019;322:312-4.[PubMed Abstract] -
- 14.Stevens CE, Taylor PE, Tong MJ, et al. Yeast-recombinant hepatitis B vaccine. Efficacy with hepatitis B immune globulin in prevention of perinatal hepatitis B virus transmission. JAMA. 1987;257:2612-6.[PubMed Abstract] -
- 15.Xu ZY, Liu CB, Francis DP, et al. Prevention of perinatal acquisition of hepatitis B virus carriage using vaccine: preliminary report of a randomized, double-blind placebo-controlled and comparative trial. Pediatrics. 1985;76:713-8.[PubMed Abstract] -
- 16.Stevens CE, Toy PT, Tong MJ, et al. Perinatal hepatitis B virus transmission in the United States. Prevention by passive-active immunization. JAMA. 1985;253:1740-5.[PubMed Abstract] -
- 17.Schillie S, Walker T, Veselsky S, et al. Outcomes of infants born to women infected with hepatitis B. Pediatrics. 2015;135:e1141-7.[PubMed Abstract] -
- 18.Boucheron P, Lu Y, Yoshida K, et al. Accuracy of HBeAg to identify pregnant women at risk of transmitting hepatitis B virus to their neonates: a systematic review and meta-analysis. Lancet Infect Dis. 2021;21:85-96.[PubMed Abstract] -
- 19.Yao N, Fu S, Wu Y, et al. Incidence of mother-to-child transmission of hepatitis B in relation to maternal peripartum antiviral prophylaxis: A systematic review and meta-analysis. Acta Obstet Gynecol Scand. 2022;101:1197-1206.[PubMed Abstract] -
- 20.Burk RD, Hwang LY, Ho GY, Shafritz DA, Beasley RP. Outcome of perinatal hepatitis B virus exposure is dependent on maternal virus load. J Infect Dis. 1994;170:1418-23.[PubMed Abstract] -
- 21.Lu Y, Song Y, Zhai X, et al. Maternal hepatitis B e antigen can be an indicator for antiviral prophylaxis of perinatal transmission of hepatitis B virus. Emerg Microbes Infect. 2021;10:555-564.[PubMed Abstract] -
- 22.Lee C, Gong Y, Brok J, Boxall EH, Gluud C. Hepatitis B immunisation for newborn infants of hepatitis B surface antigen-positive mothers. Cochrane Database Syst Rev. 2006;:CD004790.[PubMed Abstract] -
- 23.Giles ML, Visvanathan K, Lewin SR, Sasadeusz J. Chronic hepatitis B infection and pregnancy. Obstet Gynecol Surv. 2012;67:37-44.[PubMed Abstract] -
- 24.Zhang SL, Yue YF, Bai GQ, Shi L, Jiang H. Mechanism of intrauterine infection of hepatitis B virus. World J Gastroenterol. 2004;10:437-8.[PubMed Abstract] -
- 25.Xu DZ, Yan YP, Zou S, et al. Role of placental tissues in the intrauterine transmission of hepatitis B virus. Am J Obstet Gynecol. 2001;185:981-7.[PubMed Abstract] -
- 26.Xu DZ, Yan YP, Choi BC, et al. Risk factors and mechanism of transplacental transmission of hepatitis B virus: a case-control study. J Med Virol. 2002;67:20-6.[PubMed Abstract] -
- 27.Towers CV, Asrat T, Rumney P. The presence of hepatitis B surface antigen and deoxyribonucleic acid in amniotic fluid and cord blood. Am J Obstet Gynecol. 2001;184:1514-8.[PubMed Abstract] -
- 28.Chen Y, Wang L, Xu Y, et al. Role of maternal viremia and placental infection in hepatitis B virus intrauterine transmission. Microbes Infect. 2013;15:409-15.[PubMed Abstract] -
- 29.Tran TT. Hepatitis B in Pregnancy. Clin Infect Dis. 2016;62 Suppl 4:S314-7.[PubMed Abstract] -
- 30.Bai X, Yang H, Wan L, et al. Involvement of viperin in prevention of intrauterine transmission of hepatitis B virus. APMIS. 2017;125:170-5.[PubMed Abstract] -
- 31.Wang DD, Yi LZ, Wu LN, et al. Relationship between Maternal PBMC HBV cccDNA and HBV Serological Markers and its Effect on HBV Intrauterine Transmission. Biomed Environ Sci. 2019;32:315-323.[PubMed Abstract] -
- 32.Yi W, Pan CQ, Hao J, et al. Risk of vertical transmission of hepatitis B after amniocentesis in HBs antigen-positive mothers. J Hepatol. 2014;60:523-9.[PubMed Abstract] -
- 33.Alexander JM, Ramus R, Jackson G, Sercely B, Wendel GD Jr. Risk of hepatitis B transmission after amniocentesis in chronic hepatitis B carriers. Infect Dis Obstet Gynecol. 1999;7:283-6.[PubMed Abstract] -
- 34.Jourdain G, Ngo-Giang-Huong N, Harrison L, et al. Tenofovir versus placebo to prevent perinatal transmission of hepatitis B. N Engl J Med. 2018;378:911-23.[PubMed Abstract] -
- 35.Nelson NP, Easterbrook PJ, McMahon BJ. Epidemiology of Hepatitis B Virus Infection and Impact of Vaccination on Disease. Clin Liver Dis. 2016;20:607-28.[PubMed Abstract] -
- 36.Lee SD, Lo KJ, Tsai YT, et al. Role of caesarean section in prevention of mother-infant transmission of hepatitis B virus. Lancet. 1988;2:833-4.[PubMed Abstract] -
- 37.Hu Y, Chen J, Wen J, et al. Effect of elective cesarean section on the risk of mother-to-child transmission of hepatitis B virus. BMC Pregnancy Childbirth. 2013;13:119.[PubMed Abstract] -
- 38.Pan CQ, Zou HB, Chen Y, et al. Cesarean section reduces perinatal transmission of hepatitis B virus infection from hepatitis B surface antigen-positive women to their infants. Clin Gastroenterol Hepatol. 2013;11:1349-55.[PubMed Abstract] -
- 39.Ki M, Kim BW, Baik D, Kim JH. Factors associated with hepatitis B mother-to-child transmission in a national prevention program. Clin Mol Hepatol. 2025 Jun 24. 2025. Online ahead of print.[PubMed Abstract] -
- 40.Chen LZ, Zhou WQ, Zhao SS, Liu ZY, Wen SW. A nested case-control study of maternal-neonatal transmission of hepatitis B virus in a Chinese population. World J Gastroenterol. 2011;17:3640-4.[PubMed Abstract] -
- 41.Song YM, Sung J, Yang S, Choe YH, Chang YS, Park WS. Factors associated with immunoprophylaxis failure against vertical transmission of hepatitis B virus. Eur J Pediatr. 2007;166:813-8.[PubMed Abstract] -
- 42.Hill JB, Sheffield JS, Kim MJ, Alexander JM, Sercely B, Wendel GD. Risk of hepatitis B transmission in breast-fed infants of chronic hepatitis B carriers. Obstet Gynecol. 2002;99:1049-52.[PubMed Abstract] -
- 43.Beasley RP, Stevens CE, Shiao IS, Meng HC. Evidence against breast-feeding as a mechanism for vertical transmission of hepatitis B. Lancet. 1975;2:740-1.[PubMed Abstract] -
- 44.Ghaffar YA, elSobky MK, Raouf AA, Dorgham LS. Mother-to-child transmission of hepatitis B virus in a semirural population in Egypt. J Trop Med Hyg. 1989;92:20-6.[PubMed Abstract] -
- 45.Funk AL, Lu Y, Yoshida K, et al. Efficacy and safety of antiviral prophylaxis during pregnancy to prevent mother-to-child transmission of hepatitis B virus: a systematic review and meta-analysis. Lancet Infect Dis. 2021;21:70-84.[PubMed Abstract] -
- 46.Zeng QL, Zhou YH, Dong XP, et al. Expected 8-Week Prenatal vs 12-Week Perinatal Tenofovir Alafenamide Prophylaxis to Prevent Mother-to-Child Transmission of Hepatitis B Virus: A Multicenter, Prospective, Open-Label, Randomized Controlled Trial. Am J Gastroenterol. 2025;120:1045-56.[PubMed Abstract] -
- 47.Pan X, Zhou L, Hu J, et al. Tenofovir Alafenamide Therapy Throughout Pregnancy in Mothers With Hepatitis B. Aliment Pharmacol Ther. 2025;62:159-67.[PubMed Abstract] -
- 48.Pan CQ, Zhu L, Yu AS, Zhao Y, Zhu B, Dai E. Tenofovir Alafenamide Versus Tenofovir Disoproxil Fumarate for Preventing Vertical Transmission in Chronic Hepatitis B Mothers: A Systematic Review and Meta-Analysis. Clin Infect Dis. 2024;79:953-64.[PubMed Abstract] -
- 49.Li B, Liu Z, Liu X, et al. Efficacy and safety of tenofovir disoproxil fumarate and tenofovir alafenamide fumarate in preventing HBV vertical transmission of high maternal viral load. Hepatol Int. 2021;15:1103-8.[PubMed Abstract] -
- 50.Chen R, Zou J, Long L, et al. Safety and Efficacy of Tenofovir Alafenamide Fumarate in Early-Middle Pregnancy for Mothers With Chronic Hepatitis B. Front Med (Lausanne). 2022;8:796901.[PubMed Abstract] -
- 51.Ghany MG, Pan CQ, Lok AS, et al. AASLD/IDSA Practice Guideline on treatment of chronic hepatitis B. Hepatology. 2025 Nov 4. Online ahead of print.[PubMed Abstract] -
- 52.Pan CQ, Duan Z, Dai E, et al. Tenofovir to prevent hepatitis B transmission in mothers with high viral load. N Engl J Med. 2016;374:2324-34.[PubMed Abstract] -
- 53.Terrault NA, Bzowej NH, Chang KM, Hwang JP, Jonas MM, Murad MH. AASLD guidelines for treatment of chronic hepatitis B. Hepatology. 2016;63:261-83.[PubMed Abstract] -
- 54.Greenup AJ, Tan PK, Nguyen V, et al. Efficacy and safety of tenofovir disoproxil fumarate in pregnancy to prevent perinatal transmission of hepatitis B virus. J Hepatol. 2014;61:502-7.[PubMed Abstract] -
- 55.Ding Y, Cao L, Zhu L, et al. Efficacy and safety of tenofovir alafenamide fumarate for preventing mother-to-child transmission of hepatitis B virus: a national cohort study. Aliment Pharmacol Ther. 2020;52:1377-86.[PubMed Abstract] -
- 56.Chen HL, Lee CN, Chang CH, et al. Efficacy of maternal tenofovir disoproxil fumarate in interrupting mother-to-infant transmission of hepatitis B virus. Hepatology. 2015;62:375-86.[PubMed Abstract] -
- 57.Brown RS Jr, McMahon BJ, Lok AS, et al. Antiviral therapy in chronic hepatitis B viral infection during pregnancy: A systematic review and meta-analysis. Hepatology. 2016;63:319-33.[PubMed Abstract] -
- 58.Pan CQ, Dai E, Mo Z, et al. Tenofovir and Hepatitis B Virus Transmission During Pregnancy: A Randomized Clinical Trial. JAMA. 2025;333:390-9.[PubMed Abstract] -
- 59.European Association For The Study Of The Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67:370-98.[PubMed Abstract] -
- 60.Sarin SK, Kumar M, Lau GK, et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 update. Hepatol Int. 2016;10:1-98.[PubMed Abstract] -
- 61.Badell ML, Prabhu M, Dionne J, Tita ATN, Silverman NS. Society for Maternal-Fetal Medicine Consult Series #69: Hepatitis B in pregnancy: updated guidelines. Am J Obstet Gynecol. 2024;230:B2-B11.[PubMed Abstract] -
- 62.Samadi Kochaksaraei G, Castillo E, Sadler MD, et al. Real-world clinical and virological outcomes in a retrospective multiethnic cohort study of 341 untreated and tenofovir disoproxil fumarate-treated chronic hepatitis B pregnant patients in North America. Aliment Pharmacol Ther. 2020;52:1707-16.[PubMed Abstract] -
- 63.Nguyen V, Tan PK, Greenup AJ, et al. Anti-viral therapy for prevention of perinatal HBV transmission: extending therapy beyond birth does not protect against post-partum flare. Aliment Pharmacol Ther. 2014;39:1225-34.[PubMed Abstract] -
- 64.Panel on Treatment of HIV During Pregnancy and Prevention of Perinatal Transmission. Recommendations for the Use of Antiretroviral Drugs During Pregnancy and Interventions to Reduce Perinatal HIV Transmission in the United States. Recommendations for Use of Antiretroviral Drugs During Pregnancy. Lack of Experience with Antiretroviral Drugs During Pregnancy and Prior to Pregnancy (Antiretroviral-Naive). June 12, 2025.[HIV.gov] -
- 65.Takuissu GR, Kenmoe S, Amougou Atsama M, et al. Global epidemiology of occult hepatitis B virus infections in blood donors, a systematic review and meta-analysis. PLoS One. 2022;17:e0272920.[PubMed Abstract] -
- 66.Im YR, Jagdish R, Leith D, et al. Prevalence of occult hepatitis B virus infection in adults: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2022;7:932-42.[PubMed Abstract] -
- 67.Spradling PR, Xing J, Harris AM, Ly KN. Estimated Prevalence and Number of Persons With Isolated Antibody to Hepatitis B Core Antigen and Associated Occult Hepatitis B, United States, 2001-2018. J Infect Dis. 2022;225:465-69.[PubMed Abstract] -
- 68.Xie Y, Kang R, Cheng X, et al. Analysis of HBV infection characteristics and OBI prevalence in pregnant women: a focus on HBcAb + alone or in combination with HBeAb + subgroups in Northwest China. BMC Infect Dis. 2025;25:1034.[PubMed Abstract] -
- 69.Taherkhani R, Farshadpour F. Prevalence, genotype distribution and mutations of hepatitis B virus and the associated risk factors among pregnant women residing in the northern shores of Persian Gulf, Iran. PLoS One. 2022;17:e0265063.[PubMed Abstract] -
- 70.Ostankova YV, Shchemelev AN, Serikova EN, et al. Prevalence and Molecular Characterization of Chronic and Occult Hepatitis B Virus Infection Among Pregnant Women in St. Petersburg, Russia. Int J Mol Sci. 2025 Sep 18;26. Online ahead of print.[PubMed Abstract] -
- 71.Shuaib BI, Momodu A, Ohenhen JE, Umeche IE, Muhibi MA. Prevalence of overt and occult hepatitis B viral infection among pregnant women attending antenatal clinics in Edo state university teaching hospital Auchi, Nigeria. BMC Infect Dis. 2024;24:1468.[PubMed Abstract] -
- 72.Ayana DA, Mulu A, Mihret A, Seyoum B, Aseffa A, Howe R. Occult Hepatitis B virus infection among HIV negative and positive isolated anti-HBc individuals in eastern Ethiopia. Sci Rep. 2020;10:22182.[PubMed Abstract] -
- 73.Dusheiko G, Agarwal K, Maini MK. New Approaches to Chronic Hepatitis B. N Engl J Med. 2023;388:55-69.[PubMed Abstract] -
- 74.Salia E, Nartey YA, Djankpa FT, Pappoe F, Nuvor SV, Obiri-Yeboah D. Prevalence of occult hepatitis B infection among treatment-naive persons living with HIV in Ghana. PLoS One. 2024;19:e0305862.[PubMed Abstract] -
- 75.Yuen MF, Lee CK, Wong DK, et al. Prevalence of occult hepatitis B infection in a highly endemic area for chronic hepatitis B: a study of a large blood donor population. Gut. 2010;59:1389-93.[PubMed Abstract] -
- 76.Sookoian S. Liver disease during pregnancy: acute viral hepatitis. Ann Hepatol. 2006;5:231-6.[PubMed Abstract] -
- 77.Jonas MM. Hepatitis B and pregnancy: an underestimated issue. Liver Int. 2009;29 Suppl 1:133-9.[PubMed Abstract] -
- 78.Han YT, Sun C, Liu CX, et al. Clinical features and outcome of acute hepatitis B in pregnancy. BMC Infect Dis. 2014;14:368.[PubMed Abstract] -
- 79.Degertekin B, Lok AS. Indications for therapy in hepatitis B. Hepatology. 2009;49:S129-37.[PubMed Abstract] -
- 80.European Pregnancy and Paediatric HIV Cohort Collaboration (EPPICC) Study Group.. Nucleoside reverse transcriptase inhibitor backbones and pregnancy outcomes. AIDS. 2019;33:295-304.[PubMed Abstract] -
- 81.Wang L, Kourtis AP, Ellington S, Legardy-Williams J, Bulterys M. Safety of tenofovir during pregnancy for the mother and fetus: a systematic review. Clin Infect Dis. 2013;57:1773-81.[PubMed Abstract] -
- 82.Antiretroviral Pregnancy Registry Steering Committee. Antiretroviral Pregnancy Registry Interim Report for 1 January 1989 through 31 August 2022. Wilmington, NC: Registry Coordinating Center; 2022.
- 83.European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2025:S0168-8278(25)00174-6.[PubMed Abstract] -
- 84.Aebi-Popp K, Kahlert CR, Crisinel PA, et al. Transfer of antiretroviral drugs into breastmilk: a prospective study from the Swiss Mother and Child HIV Cohort Study. J Antimicrob Chemother. 2022;77:3436-42.[PubMed Abstract] -
- 85.Kayes T, Crane H, Symonds A, et al. Plasma and breast milk pharmacokinetics of tenofovir alafenamide in mothers with chronic hepatitis B infection. Aliment Pharmacol Ther. 2022;56:510-18.[PubMed Abstract] -
- 86.Yang N, Zhou G, Cheng X, et al. Distribution Evaluation of Tenofovir in the Breast Milk of Mothers With HBeAg-Positive Chronic HBV Infection After Treatment With Tenofovir Alafenamide and Tenofovir Disoproxil Fumarate by a Sensitive UPLC-MS/MS Method. Front Pharmacol. 2021;12:734760.[PubMed Abstract] -
- 87.Sylvester-Armstrong KR, Duff P. Evidence for Use of Tenofovir in Pregnancy to Prevent Perinatal Transmission of Hepatitis B Infection. Clin Obstet Gynecol. 2019;62:835-845.[PubMed Abstract] -
- 88.Mofenson LM, Baggaley RC, Mameletzis I. Tenofovir disoproxil fumarate safety for women and their infants during pregnancy and breastfeeding. AIDS. 2017 Jan 14;31:213-32.[PubMed Abstract] -
- 89.Jacobson DL, Patel K, Williams PL, et al. Growth at 2 Years of Age in HIV-exposed Uninfected Children in the United States by Trimester of Maternal Antiretroviral Initiation. Pediatr Infect Dis J. 2017;36:189-197.[PubMed Abstract] -
- 90.Siberry GK, Jacobson DL, Kalkwarf HJ, et al. Lower Newborn Bone Mineral Content Associated With Maternal Use of Tenofovir Disoproxil Fumarate During Pregnancy. Clin Infect Dis. 2015;61:996-1003.[PubMed Abstract] -
- 91.Giles M, Visvanathan K, Lewin S, et al. Clinical and virological predictors of hepatic flares in pregnant women with chronic hepatitis B. Gut. 2015;64:1810-5.[PubMed Abstract] -
- 92.Chang CY, Aziz N, Poongkunran M, et al. Serum Alanine Aminotransferase and Hepatitis B DNA Flares in Pregnant and Postpartum Women with Chronic Hepatitis B. Am J Gastroenterol. 2016;111:1410-1415.[PubMed Abstract] -
- 93.Chang CY, Aziz N, Poongkunran M, et al. Serum Aminotransferase Flares in Pregnant and Postpartum Women With Current or Prior Treatment for Chronic Hepatitis B. J Clin Gastroenterol. 2018;52:255-261.[PubMed Abstract] -
- 94.Centers for Disease Control and Prevention (CDC). Postvaccination serologic testing results for infants aged ≤24 months exposed to hepatitis B virus at birth: United States, 2008-2011. MMWR Morb Mortal Wkly Rep. 2012;61:768-71.[PubMed Abstract] -
- 95.Wong S, Chan LY, Yu V, Ho L. Hepatitis B carrier and perinatal outcome in singleton pregnancy. Am J Perinatol. 1999;16:485-8.[PubMed Abstract] -
- 96.Lobstein S, Faber R, Tillmann HL. Prevalence of hepatitis B among pregnant women and its impact on pregnancy and newborn complications at a tertiary hospital in the eastern part of Germany. Digestion. 2011;83:76-82.[PubMed Abstract] -
- 97.Safir A, Levy A, Sikuler E, Sheiner E. Maternal hepatitis B virus or hepatitis C virus carrier status as an independent risk factor for adverse perinatal outcome. Liver Int. 2010;30:765-70.[PubMed Abstract] -
- 98.Tse KY, Ho LF, Lao T. The impact of maternal HBsAg carrier status on pregnancy outcomes: a case-control study. J Hepatol. 2005;43:771-5.[PubMed Abstract] -
- 99.Tan J, Huang S, He G, et al. Maternal hepatitis B surface antigen carrier status and its impact on neonatal outcomes: a cohort study of 21 947 singleton newborns in China. J Matern Fetal Neonatal Med. 2017;30:2219-2224.[PubMed Abstract] -
- 100.Reddick KL, Jhaveri R, Gandhi M, James AH, Swamy GK. Pregnancy outcomes associated with viral hepatitis. J Viral Hepat. 2011;18:e394-8.[PubMed Abstract] -
- 101.Benaboud S, Pruvost A, Coffie PA, et al. Concentrations of tenofovir and emtricitabine in breast milk of HIV-1-infected women in Abidjan, Cote d'Ivoire, in the ANRS 12109 TEmAA Study, Step 2. Antimicrob Agents Chemother. 2011;55:1315-7.[PubMed Abstract] -
- 102.Ehrhardt S, Xie C, Guo N, Nelson K, Thio CL. Breastfeeding while taking lamivudine or tenofovir disoproxil fumarate: a review of the evidence. Clin Infect Dis. 2015;60:275-8.[PubMed Abstract] -
- 103.Mirochnick M, Taha T, Kreitchmann R, et al. Pharmacokinetics and safety of tenofovir in HIV-infected women during labor and their infants during the first week of life. J Acquir Immune Defic Syndr. 2014;65:33-41.[PubMed Abstract] -
Additional References
- Azarkar Z, Ziaee M, Ebrahimzadeh A, Sharifzadeh G, Javanmard D. Epidemiology, risk factors, and molecular characterization of occult hepatitis B infection among anti-hepatitis B core antigen alone subjects. J Med Virol. 2019;91:615-22.[PubMed Abstract] -
- Chen HL, Lin LH, Hu FC, et al. Effects of maternal screening and universal immunization to prevent mother-to-infant transmission of HBV. Gastroenterology. 2012;142:773-781.e2.[PubMed Abstract] -
- Corbett AH, Kayira D, White NR, et al. Antiretroviral pharmacokinetics in mothers and breastfeeding infants from 6 to 24 weeks post-partum: results of the BAN Study. Antivir Ther. 2014;19:587-95.[PubMed Abstract] -
- Dionne-Odom J, Tita AT, Silverman NS. #38: Hepatitis B in pregnancy screening, treatment, and prevention of vertical transmission. Am J Obstet Gynecol. 2016;214:6-14.[PubMed Abstract] -
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of liver diseases in pregnancy. J Hepatol. 2023;79:768-828.[PubMed Abstract] -
- Jourdain G, Ngo-Giang-Huong N, Cressey TR, et al. Prevention of mother-to-child transmission of hepatitis B virus: a phase III, placebo-controlled, double-blind, randomized clinical trial to assess the efficacy and safety of a short course of tenofovir disoproxil fumarate in women with hepatitis B virus e-antigen. BMC Infect Dis. 2016;16:393.[PubMed Abstract] -
- Koneru A, Fenlon N, Schillie S, Williams C, Weng MK, Nelson N. National Perinatal Hepatitis B Prevention Program: 2009-2017. Pediatrics. 2021;147:e20201823.[PubMed Abstract] -
- Koneru A, Schillie S, Roberts H, et al. Estimating Annual Births to Hepatitis B Surface Antigen-Positive Women in the United States by Using Data on Maternal Country of Birth. Public Health Rep. 2019;134:255-63.[PubMed Abstract] -
- López M, Coll O. Chronic viral infections and invasive procedures: risk of vertical transmission and current recommendations. Fetal Diagn Ther. 2010;28:1-8.[PubMed Abstract] -
- Li XM, Yang YB, Hou HY, et al. Interruption of HBV intrauterine transmission: a clinical study. World J Gastroenterol. 2003;9:1501-3.[PubMed Abstract] -
- Sagnelli E, Pisaturo M, Martini S, Filippini P, Sagnelli C, Coppola N. Clinical impact of occult hepatitis B virus infection in immunosuppressed patients. World J Hepatol. 2014;6:384-93.[PubMed Abstract] -
- Saitta C, Pollicino T, Raimondo G. Occult Hepatitis B Virus Infection: An Update. Viruses. 2022;14:1504.[PubMed Abstract] -
- Salemi JL, Spooner KK, Mejia de Grubb MC, Aggarwal A, Matas JL, Salihu HM. National trends of hepatitis B and C during pregnancy across sociodemographic, behavioral, and clinical factors, United States, 1998-2011. J Med Virol. 2017;89:1025-32.[PubMed Abstract] -
- Schillie S, Harris A, Link-Gelles R, Romero J, Ward J, Nelson N. Recommendations of the Advisory Committee on Immunization Practices for Use of a Hepatitis B Vaccine with a Novel Adjuvant. MMWR Morb Mortal Wkly Rep. 2018;67:455-8.[PubMed Abstract] -
- Wen WH, Chang MH, Zhao LL, et al. Mother-to-infant transmission of hepatitis B virus infection: significance of maternal viral load and strategies for intervention. J Hepatol. 2013;59:24-30.[PubMed Abstract] -
- Zeng QL, Yu ZJ, Ji F, et al. Tenofovir Alafenamide to Prevent Perinatal Hepatitis B Transmission: A Multicenter, Prospective, Observational Study. Clin Infect Dis. 2021;73:e3324-e3332.[PubMed Abstract] -
- Zeng QL, Zhang HX, Zhang JY, et al. Tenofovir Alafenamide for Pregnant Chinese Women With Active Chronic Hepatitis B: A Multicenter Prospective Study. Clin Gastroenterol Hepatol. 2021;S1542-3565(21)01306-9.[PubMed Abstract] -
Figures


§If anti-HBs remains <10 mIU/mL after repeat vaccination, there is no evidence of benefit for giving additional vaccine doses.







{kind=link}