Lesson 9. Screening for Hepatocellular Carcinoma
Associate Editor
Professor of Medicine
Division of Allergy & Infectious Diseases
University of Washington
Associate Editor
Associate Professor of Medicine
Division of Allergy & Infectious Diseases
University of Washington
Editor-in-Chief
Professor of Medicine
Division of Allergy & Infectious Diseases
University of Washington
Learning Objective Performance Indicators
- Describe epidemiological trends in hepatocellular carcinoma in the United States and globally
- Identify the most common risk factors for development of hepatocellular carcinoma
- Explain the rationale for proving surveillance for hepatocellular screening when indicated
- Compare and contrast hepatocellular carcinoma surveillance testing methods
- Implement guidelines for hepatocellular carcinoma screening
Epidemiology of HBV-Associated Hepatocellular Carcinoma (HCC)
Global HCC Epidemiology
Liver cancer or hepatocellular carcinoma (HCC) is the sixth most common malignancy and the third leading cause of cancer-related deaths worldwide (Figure 1).[1] In 2022, the age-standardized incidence rates for liver cancer were highest in Micronesia, Eastern Asia, and Northern Africa, at 15.1, 14.7, and 14.2 cases per 100,000 persons, respectively, whereas the United States fell into the higher intermediate category with an age-standardized rate of 6.8 cases per 100,000 persons.[1] This geographic disparity is attributable in large part to the higher prevalence of chronic hepatitis B virus (HBV) infection in Asia and Africa. Globally, chronic infection with hepatitis B virus (HBV) is the leading cause of liver cancer. Individuals with chronic HBV infection can carry a 20- to 60-fold increased risk of HCC compared to individuals without HBV infection.[2,3]
Incidence of HCC in the United States
In the United States, the Centers for Disease Control and Prevention (CDC) and the National Cancer Institute (NCI) combine hepatocellular carcinoma (HCC) and intrahepatic bile duct cancer under the category liver cancer, but HCC represents 75 to 90% of these total liver malignancies.[4,5] The annual incidence of liver cancer increased steadily from the late 1990s through 2019 and then leveled off. This overall increase in new liver cancer diagnoses is consistent with the advancing age of the United States population as a whole.[4] In 2022, there were an estimated 36,666 liver and intrahepatic bile duct cancer cases reported in the United States, according to the U.S. Cancer Statistics Working Group.[6] The rates of liver cancer and intrahepatic bile duct cancer in the United States vary significantly among different racial and ethnic groups.[4] The data on liver malignancies in the United States are summarized in the image series below (Figure 2).
HCC-Related Deaths in the United States
In 2022, liver (and intrahepatic bile duct) cancer was the sixth leading cause of cancer deaths in the United States. Consistent with the number and rate of new liver cancer cases, the number of liver cancer deaths in the United States steadily increased from 1999 through 2019, before leveling off in 2020.[4] The vast majority (greater than 90%) of liver cancer-related deaths occur among persons 55 years of age or older.[7] In 2019-2023, men had a much higher incidence of liver cancer-related deaths than women (9.4 per 100,000 men versus 4.5 per 100,000 women).[4] The liver cancer and intrahepatic bile duct cancer-related death rates in the United States varied significantly among different racial and ethnic groups.[4] The data on United States cancer-related deaths and liver cancer-related deaths are summarized in the image series below (Figure 3).
Factors that Impact HBV-Associated HCC
Factors that Increase Risk for HCC
Cirrhosis from any cause is an important risk factor for HBV-associated HCC and for HCC overall.[8,9,10,11] The reported HCC incidence in persons with cirrhosis is 2.2 to 4.3 per 100 person-years versus 0.1 to 0.8 per 100 person-years in those without cirrhosis.[12] The immune-mediated changes in the liver microenvironment and genetic damage induced by integration of HBV DNA into the host genome are thought to be contributing factors in hepatocarcinogenesis. In contrast to chronic hepatitis C virus (HCV)-related HCC, where cirrhosis is nearly ubiquitous, HBV is unique in its ability to promote tumorigenesis in the absence of cirrhosis through a variety of oncogenic mechanisms.[13,14] The integration of HBV DNA into the host cellular genome, which can induce genetic damage and stimulate HBV-associated immune-mediated changes in the liver microenvironment, is thought to be a contributing factor in hepatocarcinogenesis.[15] Most studies involving persons with HBV, however, have shown that the risk of HCC is orders of magnitude higher in the presence of cirrhosis in both treated and untreated individuals.[11,16] In addition to liver disease severity, several other factors have been associated with an increased risk of HCC:
- Older Age: Multiple studies from different regions of the world have shown that older persons with chronic HBV have a significantly higher risk of developing HCC than younger persons with chronic HBV.[16] Further, a study in the United States that utilized National Veterans Administration data showed that even in the absence of cirrhosis, HCC risk was high among persons with chronic HBV who had high alanine aminotransferase (ALT) levels and were older than 40 years of age, irrespective of their race.[17]
- Male Sex: The risk of HCC is elevated in men, at an approximately 2- to 4-fold higher risk compared with women.[18]
- Heavy Alcohol Use: Heavy alcohol use (definitions for this vary by study) has also been shown to correlate with HCC risk.[19] In an Italian case-control study, investigators reported that persons with chronic HBV increased their risk of developing HCC if they were drinking more than 60 grams of alcohol per day.[20]
- Smoking: There have also been many studies showing evidence to support an association between tobacco smoking and the risk of HCC.[21] A large study using pooled data from 14 United States-based cohort studies showed that smoking more than 25 cigarettes per day was associated with a 55% increased risk of HCC.[22]
- Obesity and/or Diabetes Mellitus: Other key host factors include the presence of obesity and/or diabetes mellitus, which may serve as a surrogate for metabolic dysfunction-associated steatotic liver disease (MASLD), an increasingly important driver of HCC in the United States and Asia.[23,24]
- Family History of HCC: A family history of HCC is also associated with a moderately increased risk of HCC, particularly among persons from Asia who have a first-degree relative with HCC.[14,25,26]
- Aflatoxin Exposure: Dietary exposure to aflatoxin is probably the strongest single environmental risk factor for HCC development that has been identified. Aflatoxin is a mycotoxin that originates from fungal contamination of staple foods (typically grains) in tropical and subtropical regions, particularly in sub-Saharan Africa and Southeast Asia. Epidemiologic data have shown a strong association between such exposure and DNA mutations of the tumor suppressor gene TP53 in chronic hepatitis B-associated HCC.[27]
- High HBV DNA Levels: Among the virologic factors that may be unfavorable for HCC, active viral replication and higher HBV DNA levels have been shown to be associated, in a dose-dependent manner, with a greater risk of HCC.[28]
- Hepatitis B e Antigen-Positive Status: Several studies have shown a correlation between positive hepatitis B e antigen (HBeAg) status and increased risk for HCC.[29,30,31] The presence of HBeAg serves as a marker for active viral replication.
- HBV Genotype C: Multiple population studies have shown an increased risk of developing HCC in persons with HBV genotype C, but infection with this genotype has not been well established outside of Asia.[25] In a study that evaluated Taiwanese men with HBV, infection with HBV genotype C was associated with an estimated 5-fold greater risk for HCC compared with other HBV genotypes.[25,32] The presence of HBV genotype C is also associated with higher HBV DNA levels. In Asia, HBV genotypes B and C are the predominant genotypes.[32]
- Hepatitis Delta Virus Coinfection: Hepatitis delta virus (HDV) is a defective single-stranded RNA virus that requires HBV to invade the host cell and complete its life cycle. Coinfection with HDV can exacerbate disease progression and increase the risk of cirrhosis, liver decompensation, and death. Its role in hepatocarcinogenesis is less clear, given confounding factors, but one meta-analysis noted an increased risk compared with individuals with HBV monoinfection.[33] The association was more pronounced when heterogeneity of studies was removed, and prospective cohort studies were examined.[33]
- Hepatitis C Virus Coinfection: Individuals with HBV and hepatitis C virus (HCV) coinfection have also been reported to be associated with an excess risk of HCC, which is consistent with the greater incidence of hepatic inflammation and cirrhosis that has been observed with HBV and HCV dual infection.
- HIV Coinfection: Coinfection with HIV can also increase the risk of HCC in the HBV context, possibly through HIV-related immunodeficiency and exacerbation of hepatic fibrogenesis.[34] This excess risk, however, is likely dependent on the degree of HBV control, presence of cirrhosis, and other cofactors.[35]
Protective Factors
There are a few factors that have been shown to reduce the risk of HCC, specifically in the context of hepatitis B.
- Primary Prevention of HBV: Primary prevention of HCC can also be accomplished through HBV vaccination. When used broadly to prevent perinatal HBV transmission, HBV immunization was the first vaccine shown to have a population-level impact on cancer prevention by reducing the cumulative risk of HCC.[36]
- Treatment of Chronic HBV: The process of hepatitis e seroconversion (change from positive HBeAg to negative HBeAg in conjunction with change from negative anti-HBe to positive anti-HBe) and sustained HBV viral suppression with antiviral therapy has been shown to reduce but not eliminate the risk of HCC.[11,15,37,38] The HBV treatment-related risk reduction for HCC has been best shown with the oral antivirals entecavir and tenofovir DF.[37,39,40,41] Because treatment reduces but does not eliminate risk for HCC, screening should continue for HCC in treated patients.
- Hepatitis B Surface Antigen Loss: The loss of hepatitis B surface antigen (HBsAg), either through treatment or spontaneous clearance, is also associated with substantially lower risk of HCC compared with persistent HBsAg positivity.[42] Residual HCC risk likely remains in those with cirrhosis, family history of HCC, coinfections, male sex, and age older than 50 years.[43,44,45]
Prognosis of Persons Diagnosed with HCC
The overall prognosis for persons diagnosed with HCC in the United States has slightly improved in the past 15 years, but it remains poor, with an overall 5-year relative survival of only approximately 22%.[6,10,46,47] This continued poor outcome is largely because individuals with HCC often present with advanced stages of cancer.[6,10] The earlier the cancer is identified, when it is localized to the liver only, the more amenable it is to local ablative therapies and the better the odds of survival. The 5-year relative survival rate drops considerably once regional (extension to lymph nodes) or metastatic cancer to distant sites occurs (Figure 4).[6,9,10] Symptoms associated with HCC, which may include abdominal pain, anorexia, early satiety, weight loss, obstructive jaundice, fever, ascites, and bone pain (from metastases), usually suggest the presence of advanced disease.[10]
Benefit of HCC Screening in Persons with HBV
Rationale for HCC Screening
The rationale for HCC screening of asymptomatic patients is that this practice may detect tumors at an early stage when potentially curative treatment, either surgical or locoregional, can be offered.[9,10,47,48] Early detection of HCC is particularly important, given the very poor prognosis associated with advanced or metastatic disease.[9,10,49,50]
Definition of Screening and Surveillance
Screening a patient for HCC means that the patient has no symptoms, and the clinician does not have a reason to suspect the patient has HCC. With screening, the patient is asymptomatic but undergoes testing to detect HCC early, before symptoms develop.[47] Surveillance is the process of serial screening test to detect the presence of HCC before it becomes clinically suspected or evident.[47] These terms have been used interchangeably, but the term surveillance can also be used to describe monitoring and follow-up of HCC after treatment. Therefore, to minimize ambiguity, the term screening will be used henceforth except in the context of specific recommendations from professional organizations.
Evidence Supporting HCC Screening in Chronic Hepatitis B
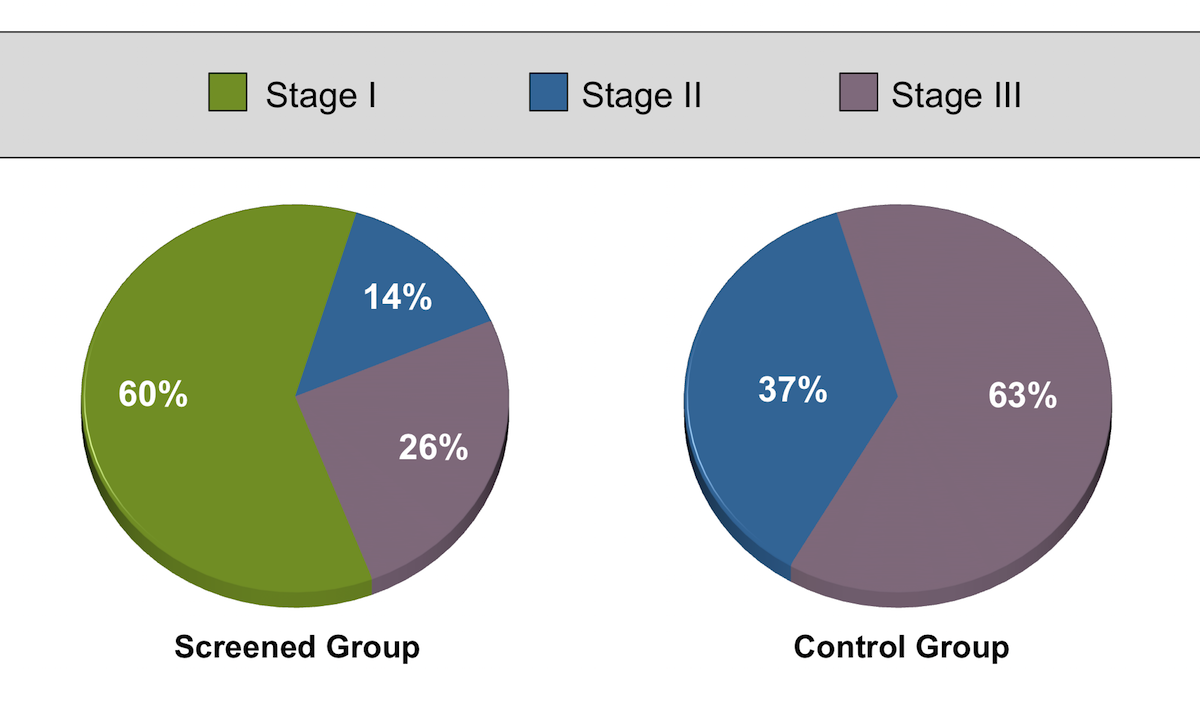
The most well-known clinical study to support HCC screening is a cluster-randomized, controlled trial conducted in China that assessed the impact of HCC screening on HCC-related mortality.[51] This study enrolled 18,816 individuals with chronic HBV aged 35 to 59 from 300 factories, businesses and schools in urban Shanghai. Half of these 300 units (n = 9,373 individuals) were randomized to screening using serum alpha-fetoprotein (AFP), with a cutoff value of 20 ng/mL, and ultrasound every 6 months; the other arm (n=9,443) underwent usual care without screening and were not actively followed.[51] The screening group had only a 58% compliance with screening, but notably had HCC diagnosed at an earlier stage, and this group had a lower HCC-related 5-year mortality rate compared with the control group (83.2 versus 131.5 per 100,000 person-years; rate ratio 0.63, 95% CI 0.41-0.98) (Figure 5).[51] This study, however, had some methodological limitations that conferrred a high risk of bias.[52] A number of observational cohort studies, a meta-analysis, and a small matched case-control trial have since suggested a survival benefit with screening, but the quality of this evidence is limited by selection, lead time, and length-time biases.[53,54,55] There are also several observational trials and reviews involving patients with cirrhosis that have shown surveillance for HCC was associated with early-stage tumor detection and improved survival.[51,53,56] Despite the suboptimal quality of evidence supporting HCC screening, it is currently the standard of practice, and it is unlikely that a rigorously conducted randomized study would take place given the widespread acceptance of screening at this time.
Implementation of HCC Screening
In the United States, several potential barriers have been identified for effective HCC screening in patients with chronic HBV infection, including undiagnosed chronic HBV infection, unknown hepatic fibrosis stage, lack of clinician awareness of HCC screening guidelines, scheduling logistics, and cost of screening.[57,58,59] Current guidelines recommend HCC screening in the context of chronic hepatitis B for patients with a variety of risk factors that include but are not exclusive to cirrhosis. It is up to the clinician to first identify these patients and then assess their risk based on these multiple features that can be challenging in non-expert settings.
HCC Surveillance Testing Methods
Serum Biomarker Tests
In general, existing serum biomarkers have a limited role in surveillance or diagnosis of HCC due to some inherent limitations in accurate early detection. The following discussion highlights currently available assays.
- Alpha-Fetoprotein: Serum alpha-fetoprotein (AFP) is the most widely evaluated biomarker for HCC surveillance, but this test has some significant drawbacks that limit it as an effective HCC screening test and high-specificity tumor marker. Using a threshold value of greater than 20 ng/mL for detecting HCC, this test has a sensitivity of only 60% and a specificity of 90%.[14,60] The AFP test on its own performs suboptimally compared to hepatic ultrasound for HCC screening.[61] The poor sensitivity is in part due to (1) the lack of uniform secretion of AFP by HCC tumors, particularly tumors less than 3 cm2, (2) the limited specificity due to fluctuating AFP levels in patients with viral hepatitis, and (3) elevated AFP levels in patients with advanced fibrotic liver disease without HCC.[62] Some experts have suggested that AFP can be useful for the diagnosis of HCC if the level is extremely elevated, but very few patients with HCC have extremely elevated AFP levels at screening. For these reasons, AFP is not recommended as the only routine surveillance test.[53,61,63] In contrast to a single threshold AFP, longitudinal changes in AFP or serial testing of AFP have been reported to increase sensitivity and specificity for detecting HCC, although this approach is not yet recommended as routine clinical practice.[64,65]
- Des-Gamma-Carboxy Prothrombin: Des-gamma-carboxy prothrombin (DCP) has been used widely in Japan for HCC diagnosis and surveillance.[66] The protein DCP is an abnormal prothrombin molecule that forms in malignant hepatocytes as a result of an acquired defect in the post-translational carboxylation of the prothrombin precursor, similar to the deficit in vitamin K deficiency; DCP is also known as the Protein Induced by Vitamin K Absence-II (PIVKA-II).[67] Experience with DCP in other countries, specifically the United States, remains limited.[68]
- Lens Culinaris Lectin-Binding Subfraction of AFP: The Lens Culinaris Lectin-Binding Subfraction of AFP (AFP-L3%) assay measures a subfraction of the AFP, which has been shown to be more specific though less sensitive than AFP.[14] Both of these biomarkers are approved by the United States Food and Drug Administration for HCC risk stratification, but not for HCC screening or surveillance.
- Liquid Biopsy: Given the low sensitivity of currently available biomarkers, there is active development of novel assays to identify circulating cell-free tumor DNA, circulating tumor cells, and circulating exosomes that can aid in the early detection of HCC, but “liquid biopsy” for HCC detection remains investigational at this time.[69]
Radiographic Imaging
Currently, ultrasound remains the cornerstone method for HCC surveillance. The following discussion reviews why ultrasound remains the recommended modality over other imaging techniques.
- Hepatic Ultrasound: Hepatic ultrasound, when performed by an operator with expertise, has a sensitivity of 60 to 80% and a specificity greater than 90% for overall detection of HCC at any stage.[66,70,71] Screening with ultrasound every 6 months has been shown to be the optimal interval both from the standpoint of cost-effectiveness and sensitivity for early-stage tumors (determined by mean HCC doubling time).[67,72,73] The interpretation of hepatic ultrasound is operator-dependent and can, at times, be difficult. For example, it can be challenging to detect a new lesion in patients with significant truncal obesity or in those who have a markedly echogenic (bright-looking) and/or heterogeneous liver, such as in those with significant fatty liver or nodular cirrhosis.[74] Guidelines have been developed to standardize the interpretation and reporting in the context of HCC screening.[75] A 1 cm size threshold is used to determine whether a lesion is considered potentially positive, as those under 1 cm are rarely malignant, whereas lesions 1 cm or larger are easier to diagnose reliably and have greater risk of representing HCC.
- Computed Tomographic Abdominal Scan: Computed Tomographic (CT) scanning of the abdomen (either with standard or multiphase contrast) is not recommended for use as a routine HCC surveillance test, given the paucity of data to support its use for screening and the potential harms associated with recurrent radiation exposure and false-positive results.[76,77] For patients who have a liver nodule greater than 1 cm detected on ultrasound, a dynamic 4-phase (not enhanced, arterial, venous, and delayed) contrast-enhanced CT scan of the liver can have diagnostic value.[53,60,77] During the arterial phase, HCC lesions enhance more intensely than the surrounding liver, but the opposite is observed during the venous and washout phases (where HCC lesions have little enhancement). This characteristic feature of HCC—the presence of arterial hypervascularity (uptake) in the lesion followed by venous or delayed phase washout—is why multiphasic cross-sectional imaging (by CT or magnetic resonance imaging [MRI]) plays an important role in the diagnosis of HCC. In persons at risk for HCC, multiphase contrast CT or MRI can establish the diagnosis of HCC without the need for liver biopsy, if characteristic radiographic findings for HCC are present.
- Magnetic Resonance Imaging: Similar to recommendations for abdominal CT scanning, hepatic magnetic resonance imaging (MRI) is not recommended as a routine surveillance test. Apart from the high cost and necessity of contrast enhancement, false-positive results can occur with MRI that may trigger further diagnostic work-up and associated harms (e.g., in increased time and anxiety for the patient). For patients who have a nodule greater than 1 cm detected on ultrasound, a contrast-enhanced multiphasic MRI is recommended as a diagnostic (as opposed to surveillance) test.[53] Further research needs to be done to evaluate the cost-effectiveness of safer modalities of MRI (such as abbreviated MRI protocols) for screening, which may be necessary for those patients in whom ultrasound performs poorly due to significant truncal obesity or marked parenchymal heterogeneity in the liver.[77]
Risk Scores to Guide Selection of Patients for HCC Surveillance
A variety of risk scores have been developed to predict the risk of HCC in patients with chronic hepatitis B, such as the REACH-B, GAG-HCC, and PAGE-B.[78,79,80] Except for the PAGE-B, many of these scoring systems were derived from individuals who were not being treated for their chronic hepatitis B and/or from Asian populations, which comprise only a subset of HBV patients in care today, thus limiting the generalizability and applicability of these risk calculators.[13] In addition to the need for further external validation in different ethnicities and populations, the determination of the appropriate risk cutoffs and associated management strategies based on these cutoffs also remains an issue at this time. Current guidelines do not endorse these scoring systems for widespread adoption and use.
Guidelines for HCC Surveillance
HCC Screening Indications
Decision analysis/cost-effectiveness models for HCC surveillance have shown that screening effectiveness depends on the incidence of HCC, with surveillance becoming cost-effective if the HCC incidence is at least 0.2% per year.[14,52,77,81]
AASLD 2023 HCC Guidance
For persons with chronic HBV infection, the 2023 AASLD HCC Guidance recommends HCC surveillance in all adults with cirrhosis of any etiology, including cirrhosis due to chronic HBV infection.[81] The exception, however, is patients with severely decompensated disease, specifically Child-Turcotte-Pugh class C cirrhosis, unless they are considered a liver transplantation candidate.[81] The following summarizes the 2023 AASLD HCC Guidance specific indications for HCC surveillance in HBsAg-positive adults.[81]
- Persons with cirrhosis (from any cause)
- Men older than 40 years of age from endemic countries
- Women older than 50 years from endemic countries
- Person from Africa at an earlier age (can be initiated as early as the third decade of life)
- Persons with a first-degree family member with a history of HCC
- PAGE-B score >10 (requires use of PAGE-B calculator)
AASLD/IDSA 2025 HBV Treatment Guidelines
The 2025 AASLD/IDSA HBV Treatment Guidelinealso recommends HCC screening for the following subgroups of people with chronic HBV and also addresses the question of continued surveillance in those who lose hepatitis surface antigen:[82]
-
Persons with hepatitis delta coinfection, regardless of cirrhosis status.
-
Persons with HIV coinfection: men 18 years of age and older and women 40 years of age and older
-
In persons who achieve HBsAg loss, continued HCC screening is advised for those with cirrhosis, a family history of HCC, men who lose HBsAg after 40 years of age, and women who lose HBsAg after 50 years of age.
HCC Surveillance Method
The HCC surveillance method recommended in the 2023 AASLD HCC Guidance is ultrasonography and serum AFP approximately every 6 months.[81] This is a notable change from prior AASLD HCC guidelines, where the option of adding AFP was left to the provider’s discretion.[14] The combination of ultrasound with AFP is slightly more sensitive than ultrasound alone (63% versus 50%) and was found to be the most cost-effective modality for HCC screening in one analysis.[83,84]
Follow-Up Based on HCC Screening Results
The 2023 AASLD HCC Guidance recommends the following algorithm for follow-up, after the surveillance ultrasound and the AFP test are completed.[81] The factors that determine the follow-up include the visualization score based on the US LI-RADS (Ultrasound Liver Imaging Reporting and Data System), which standardizes the reporting of ultrasound findings are reported for patients at risk of liver cancer, the size of the liver lesion, and the AFP level.
- If Vis score A (with no lesions on ultrasound) and the AFP is normal, repeat the ultrasound and AFP in 6 months.
- If Vis score B (or lesion less than 1 cm on ultrasound) and the AFP is normal, repeat the ultrasound and AFP in 3–6 months and repeat the AFP in 6 months. If results are stable, continue to repeat the ultrasound every 3–6 months and repeat the AFP every 6 months. If there is growth of the lesion, perform diagnostic contrast-enhanced multiphasic MRI or CT. Subsequent follow-up is based on the MRI/CT results.
- Vis score C (with no lesion or a lesion less than 1 cm on ultrasound): perform screening contrast-enhanced MRI or multiphasic CT; repeat ultrasound can be considered in some patients. Subsequent follow-up is based on the results of this imaging test.
- If there is a lesion greater than 1 cm on ultrasound, the AFP is greater than 20 ng/mL, or the AFP is increasing, perform diagnostic contrast-enhanced multiphasic MRI or CT. Subsequent follow-up is based on the MRI/CT results.
Summary Points
- Cirrhosis is an important risk factor for developing HCC in persons with chronic HBV infection. Other risk factors include older age, male sex, family history of HCC, heavy alcohol use, aflatoxin exposure, high HBV DNA levels, HBeAg-positive status, HBV genotype C, hepatitis delta, HCV coinfection, or HIV coinfection.
- The incidence of HBV-associated HCC can be reduced by vaccination against HBV. Treatment of chronic HBV with antiviral therapy has also been shown to be associated with reduced HCC risk.
- The overall relative 5-year survival of HCC in the United States is approximately 22%. Survival depends on the stage of HCC at the time of diagnosis, with a very poor prognosis for those with advanced or metastatic HCC.
- The primary goal of HCC surveillance is to detect disease at an early stage and therefore increase the likelihood of potentially curative therapy.
- The AASLD recommends HCC surveillance in all adults with chronic HBV infection and cirrhosis. For HBsAg-positive adults without cirrhosis, surveillance is based primarily on age and country of origin.
- The recommended HCC screening method is hepatic ultrasound and serum AFP every 6 months, with subsequent follow-up based on these results.
Citations
- 1.Ferlay J, Ervik M, Lam F, Laversanne M, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2024). Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer.[WHO] -
- 2.Beasley RP, Hwang LY, Lin CC, Chien CS. Hepatocellular carcinoma and hepatitis B virus. A prospective study of 22 707 men in Taiwan. Lancet. 1981;2:1129-33.[PubMed Abstract] -
- 3.Lavanchy D. Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J Viral Hepat. 2004;11:97-107.[PubMed Abstract] -
- 4.U.S. Cancer Statistics Working Group. U.S. Cancer Statistics Data Visualizations Tool, based on 2021 submission data (1999-2019): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute. Released in June 2022.[CDC and NCI] -
- 5.Wong MC, Jiang JY, Goggins WB, et al. International incidence and mortality trends of liver cancer: a global profile. Sci Rep. 2017;7:45846.[PubMed Abstract] -
- 6.National Cancer Institute. Surveillance, Epidemiology, and End Result Program: Cancer Stat Facts: Liver and Intrahepatic Bile Duct Cancer.[NCI] -
- 7.Tapper EB, Parikh ND. Mortality due to cirrhosis and liver cancer in the United States, 1999-2016: observational study. BMJ. 2018;362:k2817.[PubMed Abstract] -
- 8.El-Serag HB, Rudolph KL. Hepatocellular carcinoma: epidemiology and molecular carcinogenesis. Gastroenterology. 2007;132:2557-76.[PubMed Abstract] -
- 9.Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391:1301-1314.[PubMed Abstract] -
- 10.El-Serag HB. Hepatocellular carcinoma. N Engl J Med. 2011;365:1118-27.[PubMed Abstract] -
- 11.Papatheodoridis GV, Chan HL, Hansen BE, Janssen HL, Lampertico P. Risk of hepatocellular carcinoma in chronic hepatitis B: assessment and modification with current antiviral therapy. J Hepatol. 2015;62:956-67.[PubMed Abstract] -
- 12.Fattovich G, Stroffolini T, Zagni I, Donato F. Hepatocellular carcinoma in cirrhosis: incidence and risk factors. Gastroenterology. 2004;127:S35-50.[PubMed Abstract] -
- 13.Rizzo GEM, Cabibbo G, Craxì A. Hepatitis B Virus-Associated Hepatocellular Carcinoma. Viruses. 2022;14:986.[PubMed Abstract] -
- 14.Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68:723-50.[PubMed Abstract] -
- 15.Russo FP, Zanetto A, Pinto E, et al. Hepatocellular Carcinoma in Chronic Viral Hepatitis: Where Do We Stand? Int J Mol Sci. 2022;23:500.[PubMed Abstract] -
- 16.Raffetti E, Fattovich G, Donato F. Incidence of hepatocellular carcinoma in untreated subjects with chronic hepatitis B: a systematic review and meta-analysis. Liver Int. 2016;36:1239-51.[PubMed Abstract] -
- 17.Mittal S, Kramer JR, Omino R, et al. Role of Age and Race in the Risk of Hepatocellular Carcinoma in Veterans With Hepatitis B Virus Infection. Clin Gastroenterol Hepatol. 2018;16:252-9.[PubMed Abstract] -
- 18.Park JW, Chen M, Colombo M, et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: the BRIDGE Study. Liver Int. 2015;35:2155-66.[PubMed Abstract] -
- 19.Kuper H, Tzonou A, Kaklamani E, et al. Tobacco smoking, alcohol consumption and their interaction in the causation of hepatocellular carcinoma. Int J Cancer. 2000;85:498-502.[PubMed Abstract] -
- 20.Donato F, Tagger A, Gelatti U, et al. Alcohol and hepatocellular carcinoma: the effect of lifetime intake and hepatitis virus infections in men and women. Am J Epidemiol. 2002;155:323-31.[PubMed Abstract] -
- 21.IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Tobacco smoke and involuntary smoking. IARC Monogr Eval Carcinog Risks Hum. 2004;83:1-1438.[PubMed Abstract] -
- 22.Petrick JL, Campbell PT, Koshiol J, et al. Tobacco, alcohol use and risk of hepatocellular carcinoma and intrahepatic cholangiocarcinoma: The Liver Cancer Pooling Project. Br J Cancer. 2018;118:1005-12.[PubMed Abstract] -
- 23.Chen CL, Yang HI, Yang WS, et al. Metabolic factors and risk of hepatocellular carcinoma by chronic hepatitis B/C infection: a follow-up study in Taiwan. Gastroenterology. 2008;135:111-21.[PubMed Abstract] -
- 24.Welzel TM, Graubard BI, Zeuzem S, El-Serag HB, Davila JA, McGlynn KA. Metabolic syndrome increases the risk of primary liver cancer in the United States: a study in the SEER-Medicare database. Hepatology. 2011;54:463-71.[PubMed Abstract] -
- 25.Omata M, Cheng AL, Kokudo N, et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: a 2017 update. Hepatol Int. 2017;11:317-70.[PubMed Abstract] -
- 26.Omata M, Lesmana LA, Tateishi R, et al. Asian Pacific Association for the Study of the Liver consensus recommendations on hepatocellular carcinoma. Hepatol Int. 2010;4:439-74.[PubMed Abstract] -
- 27.Gouas D, Shi H, Hainaut P. The aflatoxin-induced TP53 mutation at codon 249 (R249S): biomarker of exposure, early detection and target for therapy. Cancer Lett. 2009;286:29-37.[PubMed Abstract] -
- 28.Chen CJ, Yang HI, Su J, et al. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA. 2006;295:65-73.[PubMed Abstract] -
- 29.Chen CJ, Yang HI. Natural history of chronic hepatitis B REVEALed. J Gastroenterol Hepatol. 2011;26:628-38.[PubMed Abstract] -
- 30.Yang HI, Lu SN, Liaw YF, et al. Hepatitis B e antigen and the risk of hepatocellular carcinoma. N Engl J Med. 2002;347:168-74.[PubMed Abstract] -
- 31.You SL, Yang HI, Chen CJ. Seropositivity of hepatitis B e antigen and hepatocellular carcinoma. Ann Med. 2004;36:215-24.[PubMed Abstract] -
- 32.Yu MW, Yeh SH, Chen PJ, et al. Hepatitis B virus genotype and DNA level and hepatocellular carcinoma: a prospective study in men. J Natl Cancer Inst. 2005;97:265-72.[PubMed Abstract] -
- 33.Alfaiate D, Clément S, Gomes D, Goossens N, Negro F. Chronic hepatitis D and hepatocellular carcinoma: A systematic review and meta-analysis of observational studies. J Hepatol. 2020;73:533-9.[PubMed Abstract] -
- 34.Hu J, Liu K, Luo J. HIV-HBV and HIV-HCV Coinfection and Liver Cancer Development. Cancer Treat Res. 2019;177:231-50.[PubMed Abstract] -
- 35.Kim HN, Newcomb CW, Carbonari DM, et al. Risk of HCC With Hepatitis B Viremia Among HIV/HBV-Coinfected Persons in North America. Hepatology. 2021;74:1190-1202.[PubMed Abstract] -
- 36.Chang MH, You SL, Chen CJ, et al. Long-term Effects of Hepatitis B Immunization of Infants in Preventing Liver Cancer. Gastroenterology. 2016;151:472-480.e1.[PubMed Abstract] -
- 37.Papatheodoridis GV, Idilman R, Dalekos GN, et al. The risk of hepatocellular carcinoma decreases after the first 5 years of entecavir or tenofovir in Caucasians with chronic hepatitis B. Hepatology. 2017;66:1444-1453.[PubMed Abstract] -
- 38.Yuen MF, Seto WK, Chow DH, et al. Long-term lamivudine therapy reduces the risk of long-term complications of chronic hepatitis B infection even in patients without advanced disease. Antivir Ther. 2007;12:1295-303.[PubMed Abstract] -
- 39.Ahn J, Lim JK, Lee HM, et al. Lower Observed Hepatocellular Carcinoma Incidence in Chronic Hepatitis B Patients Treated With Entecavir: Results of the ENUMERATE Study. Am J Gastroenterol. 2016;111:1297-304.[PubMed Abstract] -
- 40.Hosaka T, Suzuki F, Kobayashi M, et al. Long-term entecavir treatment reduces hepatocellular carcinoma incidence in patients with hepatitis B virus infection. Hepatology. 2013;58:98-107.[PubMed Abstract] -
- 41.Papatheodoridis GV, Sypsa V, Dalekos GN, et al. Hepatocellular carcinoma prediction beyond year 5 of oral therapy in a large cohort of Caucasian patients with chronic hepatitis B. J Hepatol. 2020;72:1088-96.[PubMed Abstract] -
- 42.Liu F, Wang XW, Chen L, Hu P, Ren H, Hu HD. Systematic review with meta-analysis: development of hepatocellular carcinoma in chronic hepatitis B patients with hepatitis B surface antigen seroclearance. Aliment Pharmacol Ther. 2016;43:1253-61.[PubMed Abstract] -
- 43.Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67:1560-99.[PubMed Abstract] -
- 44.Yang H, Bae SH, Nam H, et al. A risk prediction model for hepatocellular carcinoma after hepatitis B surface antigen seroclearance. J Hepatol. 2022;77:632-41.[PubMed Abstract] -
- 45.Yip TC, Chan HL, Wong VW, Tse YK, Lam KL, Wong GL. Impact of age and gender on risk of hepatocellular carcinoma after hepatitis B surface antigen seroclearance. J Hepatol. 2017;67:902-8.[PubMed Abstract] -
- 46.Altekruse SF, Henley SJ, Cucinelli JE, McGlynn KA. Changing hepatocellular carcinoma incidence and liver cancer mortality rates in the United States. Am J Gastroenterol. 2014;109:542-53.[PubMed Abstract] -
- 47.Momin BR, Pinheiro PS, Carreira H, Li C, Weir HK. Liver cancer survival in the United States by race and stage (2001-2009): Findings from the CONCORD-2 study. Cancer. 2017;123 Suppl 24:5059-5078.[PubMed Abstract] -
- 48.Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53:1020-2.[PubMed Abstract] -
- 49.Daher S, Massarwa M, Benson AA, Khoury T. Current and Future Treatment of Hepatocellular Carcinoma: An Updated Comprehensive Review. J Clin Transl Hepatol. 2018;6:69-78.[PubMed Abstract] -
- 50.Fateen W, Ryder SD. Screening for hepatocellular carcinoma: patient selection and perspectives. J Hepatocell Carcinoma. 2017;4:71-9.[PubMed Abstract] -
- 51.Zhang BH, Yang BH, Tang ZY. Randomized controlled trial of screening for hepatocellular carcinoma. J Cancer Res Clin Oncol. 2004;130:417-22.[PubMed Abstract] -
- 52.Kansagara D, Papak J, Pasha AS, et al. Screening for hepatocellular carcinoma in chronic liver disease: a systematic review. Ann Intern Med. 2014;161:261-9.[PubMed Abstract] -
- 53.Singal AG, Pillai A, Tiro J. Early detection, curative treatment, and survival rates for hepatocellular carcinoma surveillance in patients with cirrhosis: a meta-analysis. PLoS Med. 2014;11:e1001624.[PubMed Abstract] -
- 54.Su F, Weiss NS, Beste LA, et al. Screening is associated with a lower risk of hepatocellular carcinoma-related mortality in patients with chronic hepatitis B. J Hepatol. 2021;74:850-9.[PubMed Abstract] -
- 55.Zeng H, Cao M, Xia C, et al. Performance and effectiveness of hepatocellular carcinoma screening in individuals with HBsAg seropositivity in China: a multicenter prospective study. Nat Cancer. 2023;4:1382-94.[PubMed Abstract] -
- 56.Singal AG, Mittal S, Yerokun OA, et al. Hepatocellular Carcinoma Screening Associated with Early Tumor Detection and Improved Survival Among Patients with Cirrhosis in the US. Am J Med. 2017;130:1099-1106.e1.[PubMed Abstract] -
- 57.Goldberg DS, Taddei TH, Serper M, et al. Identifying barriers to hepatocellular carcinoma surveillance in a national sample of patients with cirrhosis. Hepatology. 2017;65:864-874.[PubMed Abstract] -
- 58.Farvardin S, Patel J, Khambaty M, et al. Patient-reported barriers are associated with lower hepatocellular carcinoma surveillance rates in patients with cirrhosis. Hepatology. 2017;65:875-884.[PubMed Abstract] -
- 59.Beal EW, Owen M, McNamara M, McAlearney AS, Tsung A. Patient-, Provider-, and System-Level Barriers to Surveillance for Hepatocellular Carcinoma in High-Risk Patients in the USA: a Scoping Review. J Gastrointest Cancer. 2022 Jul 26. Online ahead of print.[PubMed Abstract] -
- 60.Talwalkar JA, Gores GJ. Diagnosis and staging of hepatocellular carcinoma. Gastroenterology. 2004;127:S126-32.[PubMed Abstract] -
- 61.Gupta S, Bent S, Kohlwes J. Test characteristics of alpha-fetoprotein for detecting hepatocellular carcinoma in patients with hepatitis C. A systematic review and critical analysis. Ann Intern Med. 2003;139:46-50.[PubMed Abstract] -
- 62.Sherman M, Peltekian KM, Lee C. Screening for hepatocellular carcinoma in chronic carriers of hepatitis B virus: incidence and prevalence of hepatocellular carcinoma in a North American urban population. Hepatology. 1995;22:432-8.[PubMed Abstract] -
- 63.Tong MJ, Blatt LM, Kao VW. Surveillance for hepatocellular carcinoma in patients with chronic viral hepatitis in the United States of America. J Gastroenterol Hepatol. 2001;16:553-9.[PubMed Abstract] -
- 64.Tayob N, Lok AS, Do KA, Feng Z. Improved Detection of Hepatocellular Carcinoma by Using a Longitudinal Alpha-Fetoprotein Screening Algorithm. Clin Gastroenterol Hepatol. 2016;14:469-475.e2.[PubMed Abstract] -
- 65.Bird TG, Dimitropoulou P, Turner RM, et al. Alpha-Fetoprotein Detection of Hepatocellular Carcinoma Leads to a Standardized Analysis of Dynamic AFP to Improve Screening Based Detection. PLoS One. 2016;11:e0156801.[PubMed Abstract] -
- 66.Parikh A, Taouli B. Imaging of hepatocellular carcinoma: current concepts. Recent Results Cancer Res. 2013;190:33-55.[PubMed Abstract] -
- 67.Santi V, Trevisani F, Gramenzi A, et al. Semiannual surveillance is superior to annual surveillance for the detection of early hepatocellular carcinoma and patient survival. J Hepatol. 2010;53:291-7.[PubMed Abstract] -
- 68.Lok AS, Sterling RK, Everhart JE, et al. Des-gamma-carboxy prothrombin and alpha-fetoprotein as biomarkers for the early detection of hepatocellular carcinoma. Gastroenterology. 2010;138:493-502.[PubMed Abstract] -
- 69.Su YH, Kim AK, Jain S. Liquid biopsies for hepatocellular carcinoma. Transl Res. 2018;201:84-97.[PubMed Abstract] -
- 70.Ioannou GN, Splan MF, Weiss NS, McDonald GB, Beretta L, Lee SP. Incidence and predictors of hepatocellular carcinoma in patients with cirrhosis. Clin Gastroenterol Hepatol. 2007;5:938-45, 945.e1-4.[PubMed Abstract] -
- 71.Singal A, Volk ML, Waljee A, et al. Meta-analysis: surveillance with ultrasound for early-stage hepatocellular carcinoma in patients with cirrhosis. Aliment Pharmacol Ther. 2009;30:37-47.[PubMed Abstract] -
- 72.Barbara L, Benzi G, Gaiani S, et al. Natural history of small untreated hepatocellular carcinoma in cirrhosis: a multivariate analysis of prognostic factors of tumor growth rate and patient survival. Hepatology. 1992;16:132-7.[PubMed Abstract] -
- 73.Trinchet JC, Chaffaut C, Bourcier V, et al. Ultrasonographic surveillance of hepatocellular carcinoma in cirrhosis: a randomized trial comparing 3- and 6-month periodicities. Hepatology. 2011;54:1987-97.[PubMed Abstract] -
- 74.Simmons O, Fetzer DT, Yokoo T, et al. Predictors of adequate ultrasound quality for hepatocellular carcinoma surveillance in patients with cirrhosis. Aliment Pharmacol Ther. 2017;45:169-177.[PubMed Abstract] -
- 75.Fetzer DT, Rodgers SK, Harris AC, et al. Screening and Surveillance of Hepatocellular Carcinoma: An Introduction to Ultrasound Liver Imaging Reporting and Data System. Radiol Clin North Am. 2017;55:1197-1209.[PubMed Abstract] -
- 76.European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol. 2018;69:182–236.[EASL] -
- 77.Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67:358-80.[PubMed Abstract] -
- 78.Papatheodoridis G, Dalekos G, Sypsa V, et al. PAGE-B predicts the risk of developing hepatocellular carcinoma in Caucasians with chronic hepatitis B on 5-year antiviral therapy. J Hepatol. 2016;64:800-6.[PubMed Abstract] -
- 79.Yang JD, Mohamed EA, Aziz AO, et al. Characteristics, management, and outcomes of patients with hepatocellular carcinoma in Africa: a multicountry observational study from the Africa Liver Cancer Consortium. Lancet Gastroenterol Hepatol. 2017;2:103-11.[PubMed Abstract] -
- 80.Yuen MF, Tanaka Y, Fong DY, et al. Independent risk factors and predictive score for the development of hepatocellular carcinoma in chronic hepatitis B. J Hepatol. 2009;50:80-8.[PubMed Abstract] -
- 81.Singal AG, Llovet JM, Yarchoan M, et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78:1922-65.[PubMed Abstract] -
- 82.Ghany MG, Pan CQ, Lok AS, et al. AASLD/IDSA Practice Guideline on treatment of chronic hepatitis B. Hepatology. 2025 Nov 4. Online ahead of print.[PubMed Abstract] -
- 83.Parikh ND, Singal AG, Hutton DW, Tapper EB. Cost-Effectiveness of Hepatocellular Carcinoma Surveillance: An Assessment of Benefits and Harms. Am J Gastroenterol. 2020;115:1642-9.[PubMed Abstract] -
- 84.Tzartzeva K, Obi J, Rich NE, et al. Surveillance Imaging and Alpha Fetoprotein for Early Detection of Hepatocellular Carcinoma in Patients With Cirrhosis: A Meta-analysis. Gastroenterology. 2018;154:1706-18.e1.[PubMed Abstract] -
Additional References
- Akinyemiju T, Abera S, Ahmed M, et al. The Burden of Primary Liver Cancer and Underlying Etiologies From 1990 to 2015 at the Global, Regional, and National Level: Results From the Global Burden of Disease Study 2015. JAMA Oncol. 2017;3:1683-1691.[PubMed Abstract] -
- Altekruse SF, McGlynn KA, Reichman ME. Hepatocellular carcinoma incidence, mortality, and survival trends in the United States from 1975 to 2005. J Clin Oncol. 2009;27:1485-91.[PubMed Abstract] -
- Bruix J, Reig M, Sherman M. Evidence-Based Diagnosis, Staging, and Treatment of Patients With Hepatocellular Carcinoma. Gastroenterology. 2016;150:835-53.[PubMed Abstract] -
- Díaz-González Á, Forner A. Surveillance for hepatocellular carcinoma. Best Pract Res Clin Gastroenterol. 2016;30:1001-10.[PubMed Abstract] -
- Díaz-González Á, Reig M, Bruix J. Treatment of Hepatocellular Carcinoma. Dig Dis. 2016;34:597-602.[PubMed Abstract] -
- Dalton-Fitzgerald E, Tiro J, Kandunoori P, Halm EA, Yopp A, Singal AG. Practice patterns and attitudes of primary care providers and barriers to surveillance of hepatocellular carcinoma in patients with cirrhosis. Clin Gastroenterol Hepatol. 2015;13:791-8.e1.[PubMed Abstract] -
- de Martel C, Maucort-Boulch D, Plummer M, Franceschi S. World-wide relative contribution of hepatitis B and C viruses in hepatocellular carcinoma. Hepatology. 2015;62:1190-200.[PubMed Abstract] -
- El-Serag HB. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology. 2012;142:1264-1273.e1.[PubMed Abstract] -
- Johnson PJ, Pirrie SJ, Cox TF, et al. The detection of hepatocellular carcinoma using a prospectively developed and validated model based on serological biomarkers. Cancer Epidemiol Biomarkers Prev. 2014;23:144-53.[PubMed Abstract] -
- Kim WR, Loomba R, Berg T, et al. Impact of long-term tenofovir disoproxil fumarate on incidence of hepatocellular carcinoma in patients with chronic hepatitis B. Cancer. 2015;121:3631-8.[PubMed Abstract] -
- Konstantinou D, Deutsch M. The spectrum of HBV/HCV coinfection: epidemiology, clinical characteristics, viralinteractions and management. Ann Gastroenterol. 2015;28:221-8.[PubMed Abstract] -
- Liaw YF, Sung JJ, Chow WC, et al. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med. 2004;351:1521-31.[PubMed Abstract] -
- Lim YS, Han S, Heo NY, Shim JH, Lee HC, Suh DJ. Mortality, liver transplantation, and hepatocellular carcinoma among patients with chronic hepatitis B treated with entecavir vs lamivudine. Gastroenterology. 2014;147:152-61.[PubMed Abstract] -
- Lin OS, Keeffe EB, Sanders GD, Owens DK. Cost-effectiveness of screening for hepatocellular carcinoma in patients with cirrhosis due to chronic hepatitis C. Aliment Pharmacol Ther. 2004;19:1159-72.[PubMed Abstract] -
- Morgan RL, Baack B, Smith BD, Yartel A, Pitasi M, Falck-Ytter Y. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational studies. Ann Intern Med. 2013;158:329-37.[PubMed Abstract] -
- Njei B, Rotman Y, Ditah I, Lim JK. Emerging trends in hepatocellular carcinoma incidence and mortality. Hepatology. 2015;61:191-9.[PubMed Abstract] -
- Papatheodoridis GV, Dalekos GN, Yurdaydin C, et al. Incidence and predictors of hepatocellular carcinoma in Caucasian chronic hepatitis B patients receiving entecavir or tenofovir. J Hepatol. 2015;62:363-70.[PubMed Abstract] -
- Sarasin FP, Giostra E, Hadengue A. Cost-effectiveness of screening for detection of small hepatocellular carcinoma in western patients with Child-Pugh class A cirrhosis. Am J Med. 1996;101:422-34.[PubMed Abstract] -
- Sarin SK, Kumar M, Lau GK, et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 update. Hepatol Int. 2016;10:1-98.[PubMed Abstract] -
- Sharma S, Khalili K, Nguyen GC. Non-invasive diagnosis of advanced fibrosis and cirrhosis. World J Gastroenterol. 2014;20:16820-30.[PubMed Abstract] -
- Song P, Cai Y, Tang H, Li C, Huang J. The clinical management of hepatocellular carcinoma worldwide: A concise review and comparison of current guidelines from 2001 to 2017. Biosci Trends. 2017;11:389-98.[PubMed Abstract] -
- Tanaka Y, Kurbanov F, Mano S, et al. Molecular tracing of the global hepatitis C virus epidemic predicts regional patterns of hepatocellular carcinoma mortality. Gastroenterology. 2006;130:703-14.[PubMed Abstract] -
- Tang AS, Thornton K, and HBV Primary Care Workgroup. Hepatitis B Management: Guidance for the Primary Care Provider. February 25, 2020.
- Terrault NA, Lok ASF, McMahon BJ, et al. Update on Prevention, Diagnosis, and Treatment of Chronic Hepatitis B: AASLD 2018 Hepatitis B Guidance. Clin Liver Dis (Hoboken). 2018;12:33-34.[PubMed Abstract] -
- Thio CL, Seaberg EC, Skolasky R Jr, et al. HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter Cohort Study (MACS). Lancet. 2002;360:1921-6.[PubMed Abstract] -
- United States Cancer Statistics (USCS). Liver and Intrahepatic bile duct cancer, United States—2006-2015. U.S. Cancer Statistics Data Briefs, No. 5. November 2018[CDC/NCI] -
- White DL, Thrift AP, Kanwal F, Davila J, El-Serag HB. Incidence of Hepatocellular Carcinoma in All 50 United States, From 2000 Through 2012. Gastroenterology. 2017;152:812-20.e5.[PubMed Abstract] -
- World Health Organization. Cancer Fact Sheets, 2018. WHO’s International Agency for Research on Cancer.[WHO] -
- Yamashita S, Vauthey JN, Kaseb AO, et al. Prognosis of Fibrolamellar Carcinoma Compared to Non-cirrhotic Conventional Hepatocellular Carcinoma. J Gastrointest Surg. 2016;20:1725-31.[PubMed Abstract] -
- Yang HI, Yuen MF, Chan HL, et al. Risk estimation for hepatocellular carcinoma in chronic hepatitis B (REACH-B): development and validation of a predictive score. Lancet Oncol. 2011;12:568-74.[PubMed Abstract] -
- Yang JD, Addissie BD, Mara KC, et al. GALAD Score for Hepatocellular Carcinoma Detection in Comparison with Liver Ultrasound and Proposal of GALADUS Score. Cancer Epidemiol Biomarkers Prev. 2019;28:531-8.[PubMed Abstract] -
Figures